

Effect of Minimally Invasive Surfactant Therapy vs Sham Treatment on Death or Bronchopulmonary Dysplasia in Preterm Infants With Respiratory Distress Syndrome: The OPTIMIST-A Randomized Clinical Trial
- PMID: 34902013
- PMCID: PMC8715350
- DOI: 10.1001/jama.2021.21892
Effect of Minimally Invasive Surfactant Therapy vs Sham Treatment on Death or Bronchopulmonary Dysplasia in Preterm Infants With Respiratory Distress Syndrome: The OPTIMIST-A Randomized Clinical Trial
Abstract
Importance: The benefits of surfactant administration via a thin catheter (minimally invasive surfactant therapy [MIST]) in preterm infants with respiratory distress syndrome are uncertain.
Objective: To examine the effect of selective application of MIST at a low fraction of inspired oxygen threshold on survival without bronchopulmonary dysplasia (BPD).
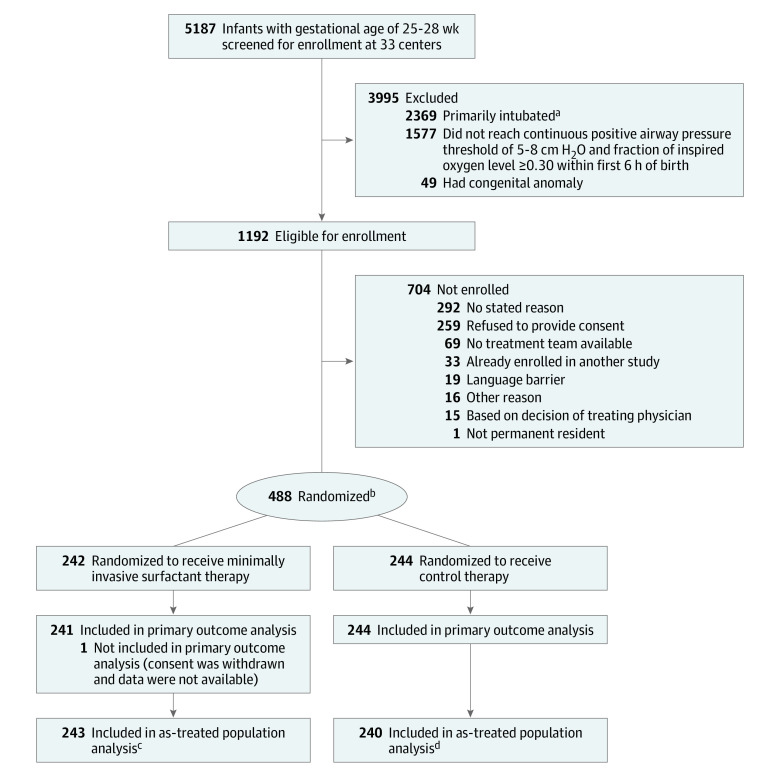
Design, setting, and participants: Randomized clinical trial including 485 preterm infants with a gestational age of 25 to 28 weeks who were supported with continuous positive airway pressure (CPAP) and required a fraction of inspired oxygen of 0.30 or greater within 6 hours of birth. The trial was conducted at 33 tertiary-level neonatal intensive care units around the world, with blinding of the clinicians and outcome assessors. Enrollment took place between December 16, 2011, and March 26, 2020; follow-up was completed on December 2, 2020.
Interventions: Infants were randomized to the MIST group (n = 241) and received exogenous surfactant (200 mg/kg of poractant alfa) via a thin catheter or to the control group (n = 244) and received a sham (control) treatment; CPAP was continued thereafter in both groups unless specified intubation criteria were met.
Main outcomes and measures: The primary outcome was the composite of death or physiological BPD assessed at 36 weeks' postmenstrual age. The components of the primary outcome (death prior to 36 weeks' postmenstrual age and BPD at 36 weeks' postmenstrual age) also were considered separately.
Results: Among the 485 infants randomized (median gestational age, 27.3 weeks; 241 [49.7%] female), all completed follow-up. Death or BPD occurred in 105 infants (43.6%) in the MIST group and 121 (49.6%) in the control group (risk difference [RD], -6.3% [95% CI, -14.2% to 1.6%]; relative risk [RR], 0.87 [95% CI, 0.74 to 1.03]; P = .10). Incidence of death before 36 weeks' postmenstrual age did not differ significantly between groups (24 [10.0%] in MIST vs 19 [7.8%] in control; RD, 2.1% [95% CI, -3.6% to 7.8%]; RR, 1.27 [95% CI, 0.63 to 2.57]; P = .51), but incidence of BPD in survivors to 36 weeks' postmenstrual age was lower in the MIST group (81/217 [37.3%] vs 102/225 [45.3%] in the control group; RD, -7.8% [95% CI, -14.9% to -0.7%]; RR, 0.83 [95% CI, 0.70 to 0.98]; P = .03). Serious adverse events occurred in 10.3% of infants in the MIST group and 11.1% in the control group.
Conclusions and relevance: Among preterm infants with respiratory distress syndrome supported with CPAP, minimally invasive surfactant therapy compared with sham (control) treatment did not significantly reduce the incidence of the composite outcome of death or bronchopulmonary dysplasia at 36 weeks' postmenstrual age. However, given the statistical uncertainty reflected in the 95% CI, a clinically important effect cannot be excluded.
Trial registration: anzctr.org.au Identifier: ACTRN12611000916943.
Conflict of interest statement
Figures
Comment in
-
Minimally Invasive Surfactant Therapy to Prevent Bronchopulmonary Dysplasia in Extremely Preterm Infants.JAMA. 2021 Dec 28;326(24):2475-2476. doi: 10.1001/jama.2021.21667. JAMA. 2021. PMID: 34901990 No abstract available.
-
EBNEO Commentary: OPTIMIST-ically moving towards targeted noninvasive surfactant therapy?Acta Paediatr. 2022 May;111(5):1091-1092. doi: 10.1111/apa.16261. Epub 2022 Jan 31. Acta Paediatr. 2022. PMID: 35100470 No abstract available.
-
Minimally Invasive Surfactant Therapy vs Sham Treatment and Death or Bronchopulmonary Dysplasia in Preterm Infants With Respiratory Distress Syndrome.JAMA. 2022 Apr 26;327(16):1613-1614. doi: 10.1001/jama.2022.2926. JAMA. 2022. PMID: 35471523 No abstract available.
-
Minimally Invasive Surfactant Therapy vs Sham Treatment and Death or Bronchopulmonary Dysplasia in Preterm Infants With Respiratory Distress Syndrome.JAMA. 2022 Apr 26;327(16):1613. doi: 10.1001/jama.2022.2923. JAMA. 2022. PMID: 35471524 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
