

Evaluation of the 3-Minute Diagnostic Confusion Assessment Method for Identification of Postoperative Delirium in Older Patients
- PMID: 34902038
- PMCID: PMC8669542
- DOI: 10.1001/jamanetworkopen.2021.37267
Evaluation of the 3-Minute Diagnostic Confusion Assessment Method for Identification of Postoperative Delirium in Older Patients
Abstract
Importance: Delirium is a common postoperative complication in older patients that often goes undetected and might lead to worse outcomes. The 3-Minute Diagnostic Confusion Assessment Method (3D-CAM) might be a practical tool for routine clinical diagnosis of delirium.
Objective: To assess the 3D-CAM for detecting postoperative delirium compared with the long-form CAM used for research purposes.
Design, setting, and participants: This cohort study of older patients enrolled in ongoing clinical trials between 2015 and 2018 was conducted at a single tertiary US hospital. Included participants were aged 60 years or older undergoing major elective surgical procedures that required at least a 2-day hospital stay. Data were analyzed between February and April 2019.
Exposures: Surgical procedures of at least 2 hours in length requiring general anesthesia with planned extubation.
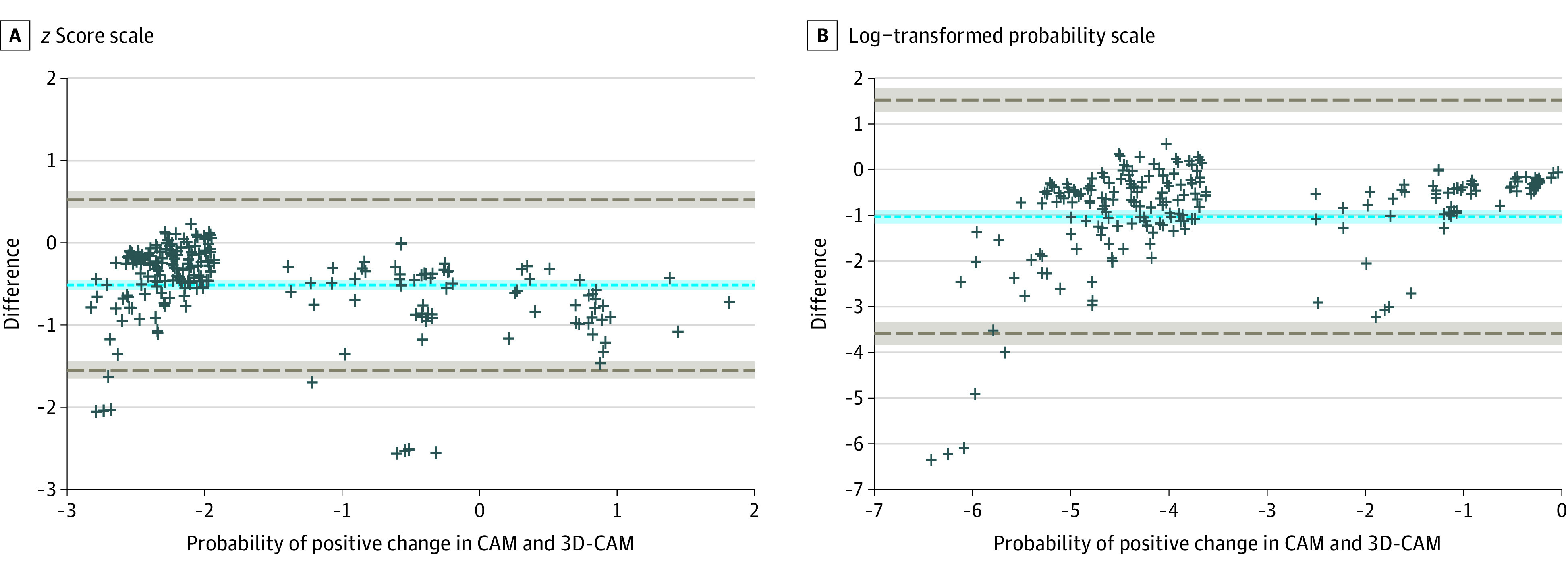
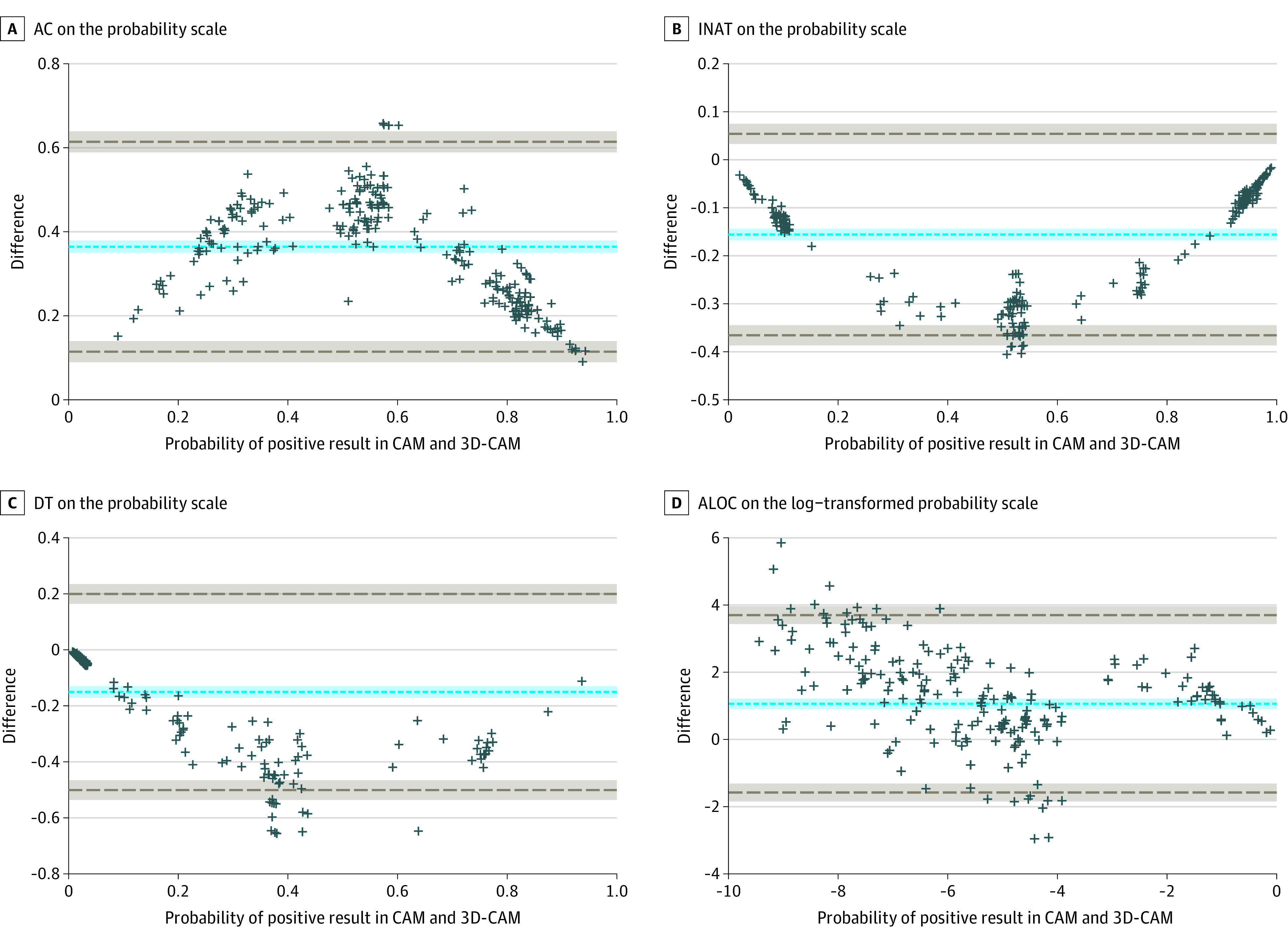
Main outcomes and measures: Patients were concurrently assessed for delirium using the 3D-CAM assessment and the long-form CAM, scored based on a standardized cognitive assessment. Agreement between these 2 methods was tested using Cohen κ with repeated measures, a generalized linear mixed-effects model, and Bland-Altman analysis.
Results: Sixteen raters conducted 471 concurrent CAM and 3D-CAM interviews including 299 patients (mean [SD] age, 69 [6.5] years), the majority of whom were men (152 [50.8%]), were White (263 [88.0%]), and had noncardiac operations (211 [70.6%]). Both instruments had good intraclass correlation (0.84 for the CAM and 0.98 for the 3D-CAM). Cohen κ demonstrated good overall agreement between the CAM and 3D-CAM (κ = 0.71; 95% CI, 0.58 to 0.83). According to the mixed-effects model, there was statistically significant disagreement between the 3D-CAM and CAM (estimated difference in fixed effect, -0.68; 95% CI, -1.32 to -0.05; P = .04). Bland-Altman analysis showed the probability of a delirium diagnosis with the 3D-CAM was more than twice the probability of a delirium diagnosis with the CAM (probability ratio, 2.78; 95% CI, 2.44 to 3.23).
Conclusions and relevance: The 3D-CAM instrument demonstrated agreement with the long-form CAM and might provide a pragmatic and sensitive clinical tool for detecting postoperative delirium, with the caveat that the 3D-CAM might overdiagnose delirium.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
