

Coronary Interventions in Pediatric Congenital Heart Disease
- PMID: 34902048
- PMCID: PMC9005385
- DOI: 10.1007/s00246-021-02784-x
Coronary Interventions in Pediatric Congenital Heart Disease
Abstract
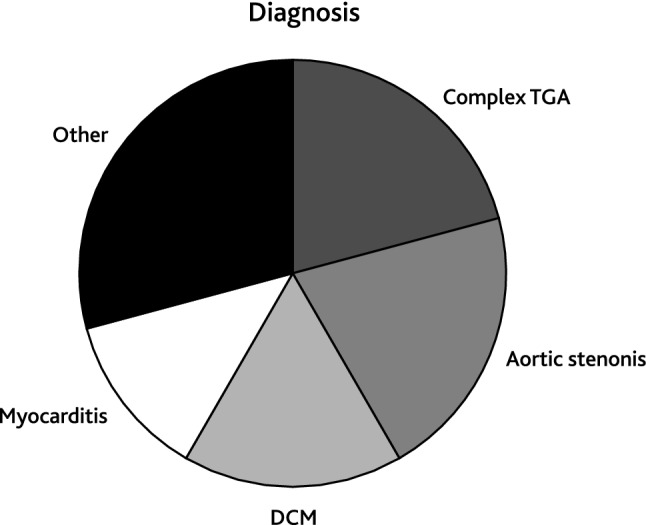
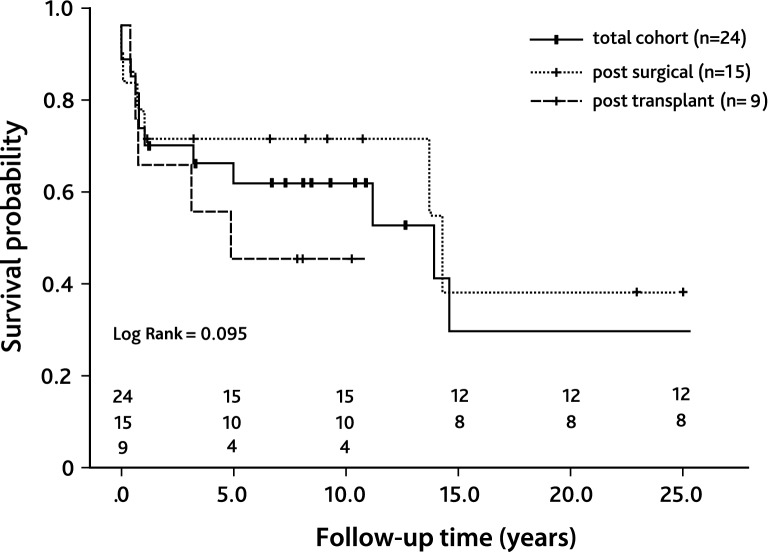
Coronary artery lesions represent rare conditions in pediatric congenital heart disease and mainly include coronary artery stenoses (CAS) or coronary artery fistulae (CAF). Due to the small vessel size, pediatric percutaneous coronary interventions (PCI) are demanding and studies concerning long-term results are missing. In this retrospective study, we analyzed indications, procedural details, and post-procedural outcomes in pediatric patients who underwent PCI in our institution. For CAS treatment, procedural success was defined as efficient coronary revascularization with a significant improvement of coronary perfusion. CAF treatment was considered successful, when no residual shunt was detectable. From 1995 to 2020, 32 pediatric patients aged ≤ 18 years received interventional treatment for CAS (n = 24/32) or CAF (n = 8/32). Reasons for CAS were post-surgical (n = 15/24) or post-transplant (n = 9/24). Interventional treatment strategies included coronary angioplasty (20/43), stent placement (10/43), and a combination of both (13/43). In-hospital mortality occurred in 6/24 patients and late mortality in 5/24 patients leading to an overall 5-year survival of 62.5%. Early mortality mainly occurred due to post-ischemic myocardial failure. CAF occlusion was performed using coil embolization (n = 3), placement of vascular plugs (n = 3), a combination of both (n = 1), or a combination of coil embolization and a covered stent (n = 1). Treatment of coronary fistulae was successful in all patients with excellent post-procedural results and no follow-up death. PCI in pediatric patients with congenital heart disease can be performed safely and effectively. However, the overall 5-year survival probability of patients with CAS is reduced due to severe ischemic myocardial damage.
Keywords: Cardiac allograft vasculopathy; Coronary artery stenosis; Coronary fistula; Pediatric congenital heart disease; Percutaneous coronary intervention.
© 2021. The Author(s).
Conflict of interest statement
All authors declare not to have any conflict of interest.
Figures


References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
