

Development and validation of a new scoring system for prognostic prediction of community-acquired pneumonia in older adults
- PMID: 34903833
- PMCID: PMC8668907
- DOI: 10.1038/s41598-021-03440-3
Development and validation of a new scoring system for prognostic prediction of community-acquired pneumonia in older adults
Abstract
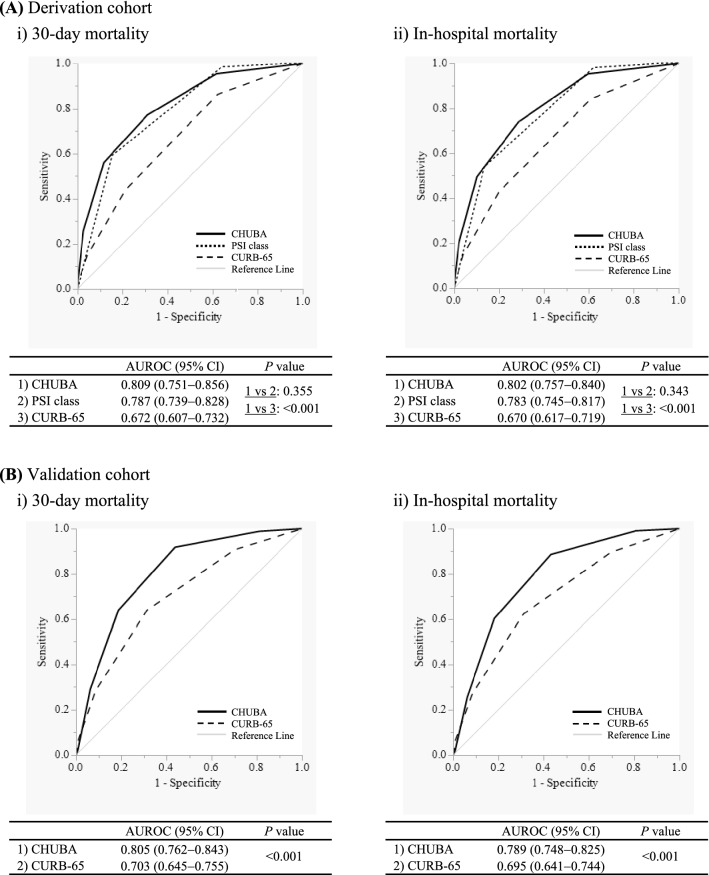
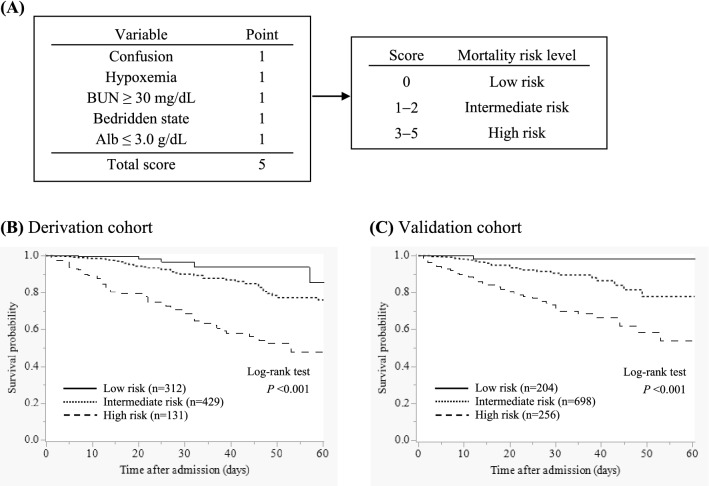
The discriminative power of CURB-65 for mortality in community-acquired pneumonia (CAP) is suspected to decrease with age. However, a useful prognostic prediction model for older patients with CAP has not been established. This study aimed to develop and validate a new scoring system for predicting mortality in older patients with CAP. We recruited two prospective cohorts including patients aged ≥ 65 years and hospitalized with CAP. In the derivation (n = 872) and validation cohorts (n = 1,158), the average age was 82.0 and 80.6 years and the 30-day mortality rate was 7.6% (n = 66) and 7.4% (n = 86), respectively. A new scoring system was developed based on factors associated with 30-day mortality, identified by multivariate analysis in the derivation cohort. This scoring system named CHUBA comprised five variables: confusion, hypoxemia (SpO2 ≤ 90% or PaO2 ≤ 60 mmHg), blood urea nitrogen ≥ 30 mg/dL, bedridden state, and serum albumin level ≤ 3.0 g/dL. With regard to 30-day mortality, the area under the receiver operating characteristic curve for CURB-65 and CHUBA was 0.672 (95% confidence interval, 0.607-0.732) and 0.809 (95% confidence interval, 0.751-0.856; P < 0.001), respectively. The effectiveness of CHUBA was statistically confirmed in the external validation cohort. In conclusion, a simpler novel scoring system, CHUBA, was established for predicting mortality in older patients with CAP.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Metlay JP, et al. Diagnosis and treatment of adults with community-acquired pneumonia. An official clinical practice guideline of the American Thoracic Society and Infectious Diseases Society of America. Am. J. Respir. Crit. Care Med. 2019;200:e45–e67. doi: 10.1164/rccm.201908-1581ST. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
