

Is endoscopic retrograde appendicitis therapy a better modality for acute uncomplicated appendicitis? A systematic review and meta-analysis
- PMID: 34904091
- PMCID: PMC8638047
- DOI: 10.12998/wjcc.v9.i33.10208
Is endoscopic retrograde appendicitis therapy a better modality for acute uncomplicated appendicitis? A systematic review and meta-analysis
Abstract
Background: Previous studies had shown endoscopic retrograde appendicitis therapy (ERAT) is an effective treatment for acute appendicitis. However, different studies reported conflicting outcomes regarding the effectiveness of ERAT in comparison with laparoscopic appendectomy (LA).
Aim: To compare the effectiveness of ERAT with LA.
Methods: Randomized controlled trials (RCTs) and retrospective studies of ERAT for acute uncomplicated appendicitis were searched in PubMed, Cochrane Library, Web of Science, Embase database, China National Knowledge Infrastructure (CNKI), the WanFang Database, and Chinese Scientific Journals Database (VIP) from the establishment date to March 1 2021. Heterogeneity was assessed using the I-squared statistic. Pooled odds ratios (OR), weighted mean difference (WMD), and standard mean difference (SMD), with 95% confidence intervals (CI) were calculated through either fixed-effects or random-effects model. Sensitivity analysis was also performed. Publication bias was tested by Egger's test, and Begg's test. The quality of included RCT were evaluated by the Jadad scale, while Newcastle-Ottawa scale is adopted for assessing the methodological quality of case-control studies. All statistical analysis was performed using Stata 15.1 statistical software. All statistical analysis was performed using Stata 15.1 statistical software. This study is registered with PROSPERO, CRD42021243955.
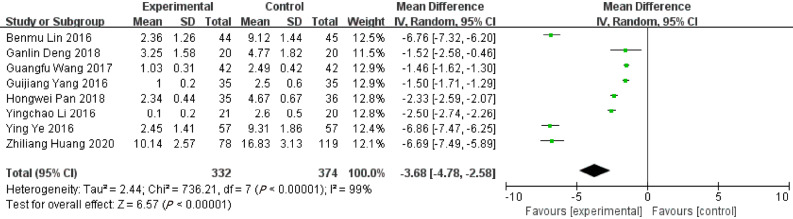
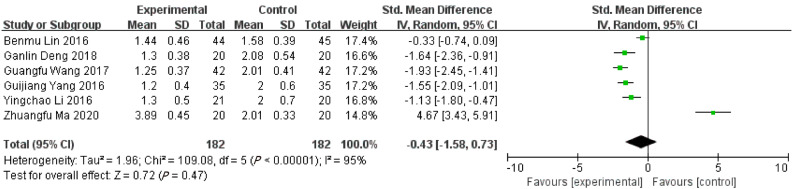
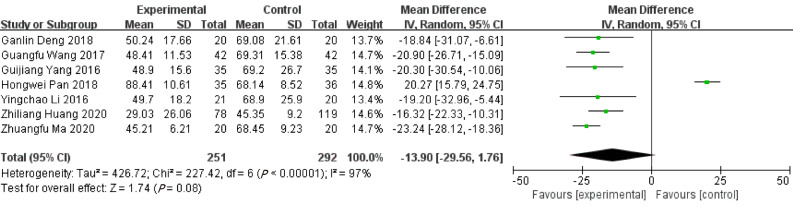
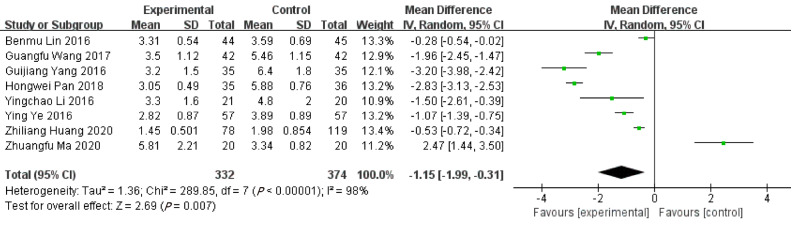
Results: After screening, 10 RCTs and 2 case-control studies were included in the current systematic review. Firstly, the length of hospitalizations [WMD = -1.15, 95%CI: -1.99, -0.31; P = 0.007] was shorter than LA group. Secondly, the level of post-operative CRP [WMD = -10.06, 95%CI: (-17.39, -2.73); P = 0.007], TNF-α [WMD = -7.70, 95%CI: (-8.47, -6.93); P < 0.001], and IL-6 Levels [WMD = -9.78, 95%CI: (-10.69, -8.88); P < 0.001; P < 0.001] in ERAT group was significantly lower than LA group. Thirdly, ERAT group had a lower incidence of intestinal obstruction than LA group. [OR = 0.19, 95%CI: (0.05, 0.79); P = 0.020]. Moreover, the quality of 10 RCTs were low with 0-3 Jadad scores, while the methodological quality of two case-control studies were fair with a score of 2 (each).
Conclusion: Compared with LA, ERAT reduces operation time, the level of postoperative inflammation, and results in fewer complications and shorter recovery time, with preserving the appendix and its immune and biological functions.
Keywords: Acute appendicitis; Endoscopic retrograde appendicitis therapy; Laparoscopic appendectomy; Meta analysis; Randomized controlled study.
©The Author(s) 2021. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: Allauthors have no conflict(s) of interest to declare in relation to this manuscript.
Figures

References
-
- Alore EA, Ward JL, Rob TS. Population-level outcomes of early versus delayed appendectomy for acute appendicitis using the American College of Surgeons National Surgical Quality Improvement Program. J Surg Res . 2018:229: 234–242. - PubMed
-
- Rentea RM, Peter SDS, Snyder CL. Pediatric appendicitis: state of the art review. Pediatr Surg Int . 2017;33:269–283. - PubMed
-
- Fagerström A, Paajanen P, Saarelainen H, Ahonen-Siirtola M, Ukkonen M, Miettinen P, Paajanen H. Non-specific abdominal pain remains as the most common reason for acute abdomen: 26-year retrospective audit in one emergency unit. Scand J Gastroenterol . 2017;52:1072–1077. - PubMed
-
- Georgiou R, Eaton S, Stanton MP, Pierro A, Hall NJ. Efficacy and Safety of Nonoperative Treatment for Acute Appendicitis: A Meta-analysis. Pediatrics . 2017;139 - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
