

First Clinical Photon-counting Detector CT System: Technical Evaluation
- PMID: 34904876
- PMCID: PMC8940675
- DOI: 10.1148/radiol.212579
First Clinical Photon-counting Detector CT System: Technical Evaluation
Abstract
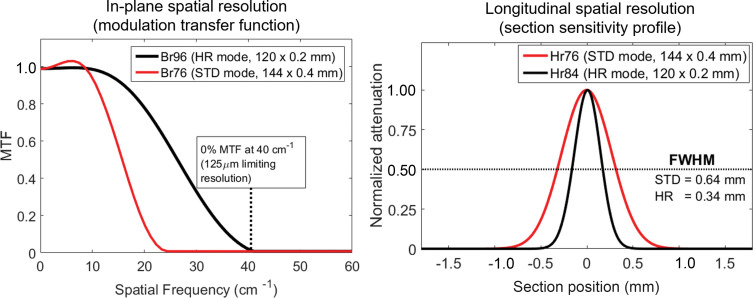
Background The first clinical CT system to use photon-counting detector (PCD) technology has become available for patient care. Purpose To assess the technical performance of the PCD CT system with use of phantoms and representative participant examinations. Materials and Methods Institutional review board approval and written informed consent from four participants were obtained. Technical performance of a dual-source PCD CT system was measured for standard and high-spatial-resolution (HR) collimations. Noise power spectrum, modulation transfer function, section sensitivity profile, iodine CT number accuracy in virtual monoenergetic images (VMIs), and iodine concentration accuracy were measured. Four participants were enrolled (between May 2021 and August 2021) in this prospective study and scanned using similar or lower radiation doses as their respective clinical examinations performed on the same day using energy-integrating detector (EID) CT. Image quality and findings from the participants' PCD CT and EID CT examinations were compared. Results All standard technical performance measures met accreditation and regulatory requirements. Relative to filtered back-projection reconstructions, images from iterative reconstruction had lower noise magnitude but preserved noise power spectrum shape and peak frequency. Maximum in-plane spatial resolutions of 125 and 208 µm were measured for HR and standard PCD CT scans, respectively. Minimum values for section sensitivity profile full width at half maximum measurements were 0.34 mm (0.2-mm nominal section thickness) and 0.64 mm (0.4-mm nominal section thickness) for HR and standard PCD CT scans, respectively. In a 120-kV standard PCD CT scan of a 40-cm phantom, VMI iodine CT numbers had a mean percentage error of 5.7%, and iodine concentration had root mean squared error of 0.5 mg/cm3, similar to previously reported values for EID CT. VMIs, iodine maps, and virtual noncontrast images were created for a coronary CT angiogram acquired with 66-msec temporal resolution. Participant PCD CT images showed up to 47% lower noise and/or improved spatial resolution compared with EID CT. Conclusion Technical performance of clinical photon-counting detector (PCD) CT is improved relative to that of a current state-of-the-art CT system. The dual-source PCD geometry facilitated 66-msec temporal resolution multienergy cardiac imaging. Study participant images illustrated the effect of the improved technical performance. © RSNA, 2022 Online supplemental material is available for this article. See also the editorial by Willemink and Grist in this issue.
Conflict of interest statement
Figures


![Images in a 71-year-old man scanned with(A) energy-integrating detector (EID) CT and (B, C) photon-counting detector (PCD) CT with dual-source geometry to achieve 66-msec temporal resolution. Axial images are shown in left column, and oblique coronal images are shown in right column. While the EID CT examination is limited to single-energy data (A) at this temporal resolution, the multienergy capabilities of the PCD CT system allowed creation of low-energy (45, 55 keV) virtual monoenergetic images (VMIs) (B), which showed increased iodine signal (shown as mean Hounsfield unit measurements in regions of interest) compared with EID CT despite an 18% decrease (A: 110 mL vs B, C: 90 mL iohexol [Omnipaque 350, GE Healthcare]) in volume of administered contrast material (mean CT numbers for the black circular regions of interest are given in the left column of images). The use of VMIs adds to the inherently higher iodine contrast-to-noise ratio possible with PCD CT and provides clearer delineation of a branch of the left coronary artery (arrowheads). Increasing the VMI energy (65 keV or higher) decreased calcium blooming relative to EID CT (arrows in A and B). Absolute iodine concentration was measured using the iodine map images (mean concentration in mg/cm3 unit shown in region of interest) and virtual noncontrast (VNC) images used to visualize calcifications (arrow in C) with attenuation similar to that of iodinated blood. Reconstruction kernels used were as follows: Bv40 (body-vascular, sharpness level 40) (EID CT 90-kV, in A), Bv48 (PCD CT VMIs in B), Qr40 (quantitative-regular, sharpness level 40) (PCD CT iodine map and VNC images in C) Display windows and levels were as follows: 2000 HU and 200 HU for EID CT and PCD CT VMIs, 30/15 mg · mL−1 for iodine map, and 1000 HU and 100 HU for VNC image.](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/ba74/8961720/2ba4137b8585/radiol.212579fig3.jpg)
![Axial images in an 85-year-old man with aortoiliac stent graft scanned for angiography with energy-integrating detector (EID) CT at 100 kV (left column) and high-spatial-resolution photon-counting detector (PCD) CT (low-energy threshold, or T3D, images; includes photon energies from 20 to 120 keV) (center and right columns). Both scans were obtained with similar radiation doses (approximately 10 mGy). Images in the top row correspond to enlarged view of the rectangular region of interest displayed in the bottom row. PCD CT image in right column was created using sharper resolution (Br72 [body-regular, sharpness level 72] kernel) than is possible to achieve with EID CT, which reduces stent blooming and improves delineation of struts at the expense of increased image noise (shown as standard deviation of pixel values in the white circular region of interest [SD]). Display window = 1800 HU; display level = 440 HU.](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/ba74/8961720/a1ef334fdd4c/radiol.212579fig4.jpg)

Comment in
-
Counting Photons: The Next Era for CT Imaging?Radiology. 2022 Apr;303(1):139-140. doi: 10.1148/radiol.213203. Epub 2022 Feb 15. Radiology. 2022. PMID: 35166591 No abstract available.
References
-
- Sartoretti T , Eberhard M , Nowak T , et al . Photon-counting multienergy computed tomography with spectrally optimized contrast media for plaque removal and stenosis assessment . Invest Radiol 2021. ; 56 ( 9 ): 563 – 570 . - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
