

Heterogeneity of Treatment Effects in an Analysis of Pooled Individual Patient Data From Randomized Trials of Device Closure of Patent Foramen Ovale After Stroke
- PMID: 34905030
- PMCID: PMC8672231
- DOI: 10.1001/jama.2021.20956
Heterogeneity of Treatment Effects in an Analysis of Pooled Individual Patient Data From Randomized Trials of Device Closure of Patent Foramen Ovale After Stroke
Erratum in
-
Data Plotted Incorrectly in Figure 2.JAMA. 2022 Jan 25;327(4):394. doi: 10.1001/jama.2021.24545. JAMA. 2022. PMID: 35076685 Free PMC article. No abstract available.
Abstract
Importance: Patent foramen ovale (PFO)-associated strokes comprise approximately 10% of ischemic strokes in adults aged 18 to 60 years. While device closure decreases stroke recurrence risk overall, the best treatment for any individual is often unclear.
Objective: To evaluate heterogeneity of treatment effect of PFO closure on stroke recurrence based on previously developed scoring systems.
Design, setting, and participants: Investigators for the Systematic, Collaborative, PFO Closure Evaluation (SCOPE) Consortium pooled individual patient data from all 6 randomized clinical trials that compared PFO closure plus medical therapy vs medical therapy alone in patients with PFO-associated stroke, and included a total of 3740 participants. The trials were conducted worldwide from 2000 to 2017.
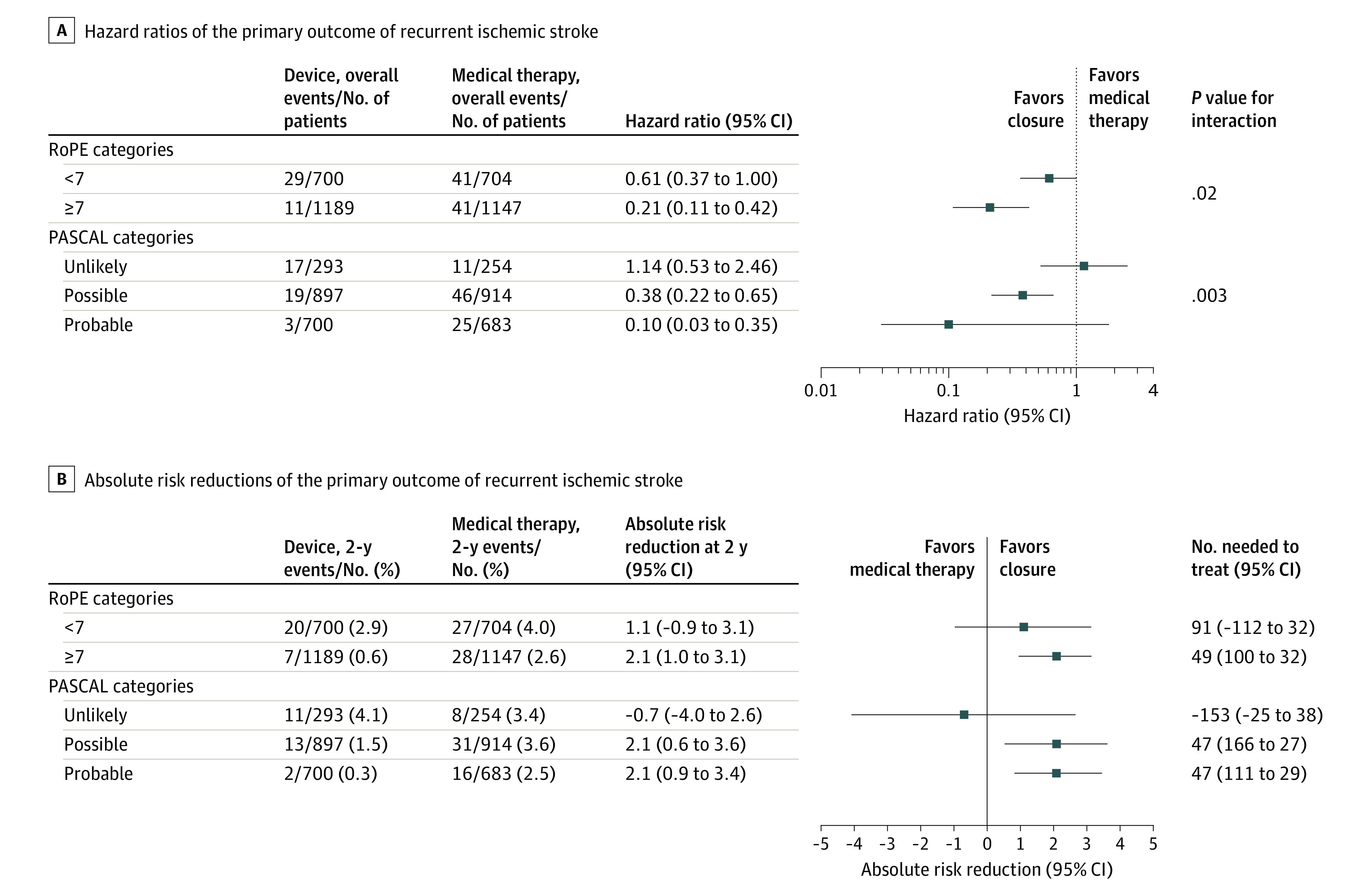
Exposures: PFO closure plus medical therapy vs medical therapy alone. Subgroup analyses used the Risk of Paradoxical Embolism (RoPE) Score (a 10-point scoring system in which higher scores reflect younger age and the absence of vascular risk factors) and the PFO-Associated Stroke Causal Likelihood (PASCAL) Classification System, which combines the RoPE Score with high-risk PFO features (either an atrial septal aneurysm or a large-sized shunt) to classify patients into 3 categories of causal relatedness: unlikely, possible, and probable.
Main outcomes and measures: Ischemic stroke.
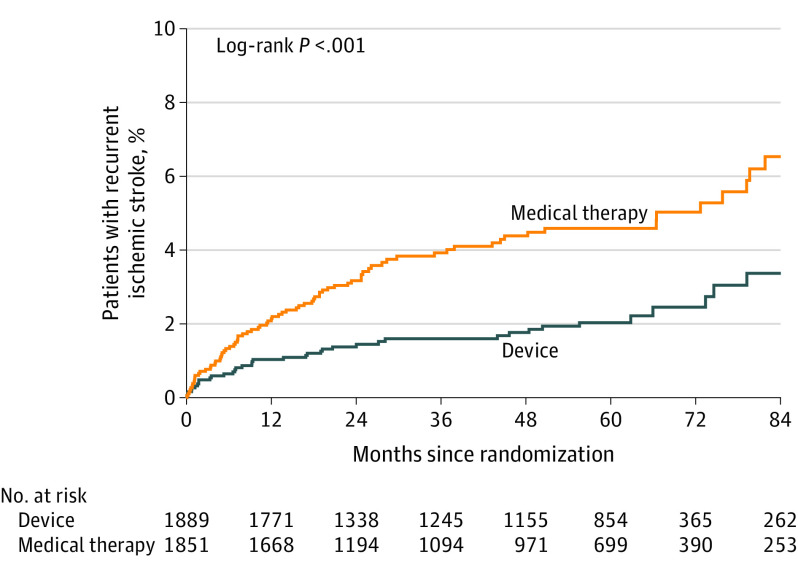
Results: Over a median follow-up of 57 months (IQR, 24-64), 121 outcomes occurred in 3740 patients. The annualized incidence of stroke with medical therapy was 1.09% (95% CI, 0.88%-1.36%) and with device closure was 0.47% (95% CI, 0.35%-0.65%) (adjusted hazard ratio [HR], 0.41 [95% CI, 0.28-0.60]). The subgroup analyses showed statistically significant interaction effects. Patients with low vs high RoPE Score had HRs of 0.61 (95% CI, 0.37-1.00) and 0.21 (95% CI, 0.11-0.42), respectively (P for interaction = .02). Patients classified as unlikely, possible, and probable using the PASCAL Classification System had HRs of 1.14 (95% CI, 0.53-2.46), 0.38 (95% CI, 0.22-0.65), and 0.10 (95% CI, 0.03-0.35), respectively (P for interaction = .003). The 2-year absolute risk reduction was -0.7% (95% CI, -4.0% to 2.6%), 2.1% (95% CI, 0.6%-3.6%), and 2.1% (95% CI, 0.9%-3.4%) in the unlikely, possible, and probable PASCAL categories, respectively. Device-associated adverse events were generally higher among patients classified as unlikely; the absolute risk increases in atrial fibrillation beyond day 45 after randomization with a device were 4.41% (95% CI, 1.02% to 7.80%), 1.53% (95% CI, 0.33% to 2.72%), and 0.65% (95% CI, -0.41% to 1.71%) in the unlikely, possible, and probable PASCAL categories, respectively.
Conclusions and relevance: Among patients aged 18 to 60 years with PFO-associated stroke, risk reduction for recurrent stroke with device closure varied across groups classified by their probabilities that the stroke was causally related to the PFO. Application of this classification system has the potential to guide individualized decision-making.
Conflict of interest statement
Figures
Comment in
-
Heterogeneity of Treatment Effect: Estimating How the Effects of Interventions Vary Across Individuals.JAMA. 2021 Dec 14;326(22):2312-2313. doi: 10.1001/jama.2021.20552. JAMA. 2021. PMID: 34905043 No abstract available.
-
Patent Foramen Ovale Closure-Harnessing Clinical Trial Evidence to Inform Individualized Treatment Decisions.JAMA. 2021 Dec 14;326(22):2265-2267. doi: 10.1001/jama.2021.21317. JAMA. 2021. PMID: 34905044 No abstract available.
-
Treatment Effects in Analysis of Pooled Individual Patient Data From Randomized Trials of Device Closure of Patent Foramen Ovale.JAMA. 2022 Apr 12;327(14):1403. doi: 10.1001/jama.2022.2658. JAMA. 2022. PMID: 35412569 No abstract available.
References
-
- Kleindorfer DO, Towfighi A, Chaturvedi S, et al. 2021 Guideline for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline from the American Heart Association/American Stroke Association. Stroke. 2021;52(7):e364-e467. doi: 10.1161/STR.0000000000000375 - DOI - PubMed
-
- Pristipino C, Sievert H, D’Ascenzo F, et al. ; Evidence Synthesis Team; Eapci Scientific Documents and Initiatives Committee; International Experts . European position paper on the management of patients with patent foramen ovale: general approach and left circulation thromboembolism. Eur Heart J. 2019;40(38):3182-3195. doi: 10.1093/eurheartj/ehy649 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
