

Technical evaluation of the cone-beam computed tomography imaging performance of a novel, mobile, gantry-based X-ray system for brachytherapy
- PMID: 34905285
- PMCID: PMC8833290
- DOI: 10.1002/acm2.13501
Technical evaluation of the cone-beam computed tomography imaging performance of a novel, mobile, gantry-based X-ray system for brachytherapy
Abstract
Purpose: A novel, mobile cone-beam computed tomography (CBCT) system for image-guided adaptive brachytherapy was recently deployed at our hospital as worldwide first site. Prior to the device's clinical operation, a profound characterization of its imaging performance was conducted. This was essential to optimize both the imaging workflow and image quality for achieving the best possible clinical outcomes. We present the results of our investigations.
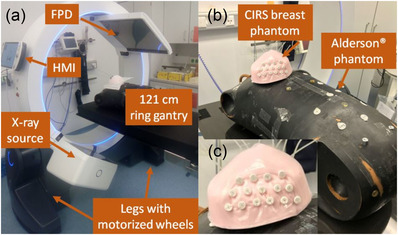
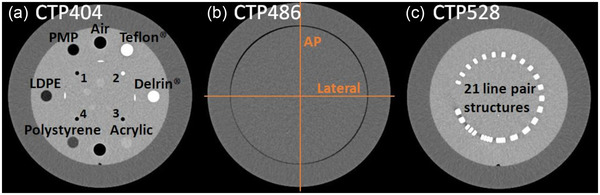
Methods: The novel CBCT-system features a ring gantry with 121 cm clearance as well as a 43.2 × 43.2 cm2 flat-panel detector, and is controlled via a tablet-personal computer (PC). For evaluating its imaging performance, the geometric reproducibility as well as imaging fidelity, computed tomography (CT)-number accuracy, uniformity, contrast-noise-ratio (CNR), noise characteristics, and spatial resolution as fundamental image quality parameters were assessed. As dose metric the weighted cone-beam dose index (CBDIw ) was measured. Image quality was evaluated using standard quality assurance (QA) as well as anthropomorphic upper torso and breast phantoms. Both in-house and manufacturer protocols for abdomen, pelvis, and breast imaging were examined.
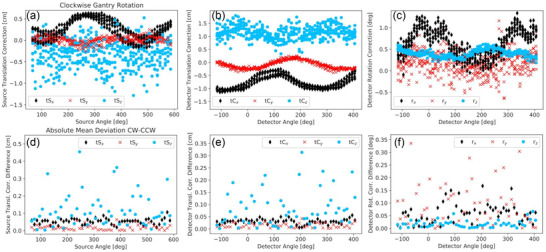
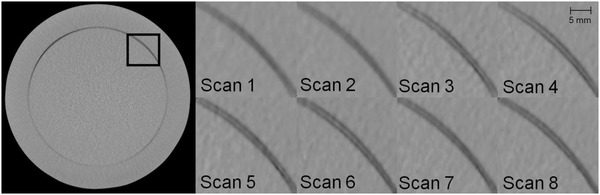
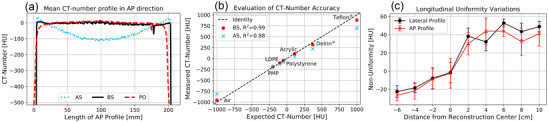
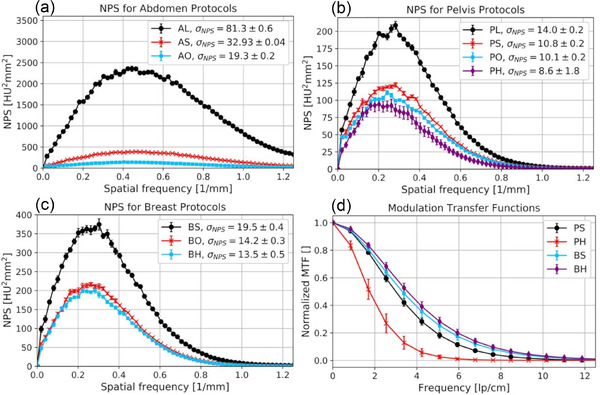
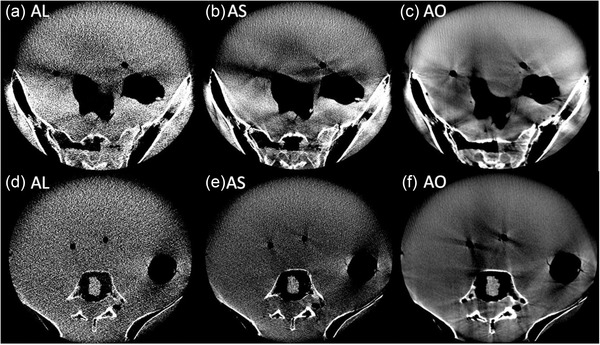
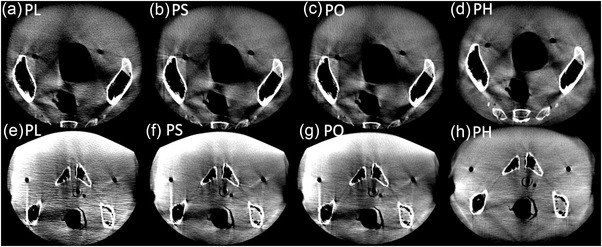
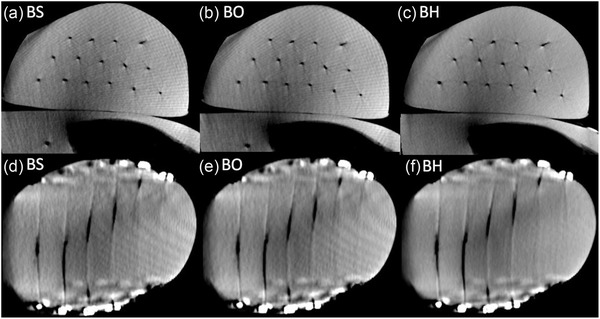
Results: Using the in-house protocols, the QA phantom scans showed altogether a high image quality, with high CT-number accuracy (R2 > 0.97) and uniformity (<12 Hounsfield Unit (HU) cupping), reasonable noise and imaging fidelity, and good CNR at bone-tissue transitions of up to 28:1. Spatial resolution was strongly limited by geometric instabilities of the device. The breast phantom scans fulfilled clinical requirements, whereas the abdomen and pelvis scans showed severe artifacts, particularly at air/bone-tissue transitions.
Conclusion: With the novel CBCT-system, achieving a high image quality appears possible in principle. However, adaptations of the standard protocols, performance enhancements in image reconstruction referring to artifact reductions, as well as the extinction of geometric instabilities are imperative.
Keywords: cone-beam computed tomography (CBCT); image quality; image-guided adaptive brachytherapy; imaging performance analysis; mobile X-ray system.
© 2021 The Authors. Journal of Applied Clinical Medical Physics published by Wiley Periodicals, LLC on behalf of The American Association of Physicists in Medicine.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Quality assurance and long-term stability of a novel 3-in-1 X-ray system for brachytherapy.J Appl Clin Med Phys. 2022 Sep;23(9):e13727. doi: 10.1002/acm2.13727. Epub 2022 Jul 18. J Appl Clin Med Phys. 2022. PMID: 35848090 Free PMC article.
-
Characterization of a prototype rapid kilovoltage x-ray image guidance system designed for a ring shape radiation therapy unit.Med Phys. 2019 Mar;46(3):1355-1370. doi: 10.1002/mp.13396. Epub 2019 Feb 13. Med Phys. 2019. PMID: 30675902 Free PMC article.
-
A mobile isocentric C-arm for intraoperative cone-beam CT: Technical assessment of dose and 3D imaging performance.Med Phys. 2020 Mar;47(3):958-974. doi: 10.1002/mp.13983. Epub 2020 Jan 6. Med Phys. 2020. PMID: 31863480 Free PMC article.
-
Technical Principles of Dual-Energy Cone Beam Computed Tomography and Clinical Applications for Radiation Therapy.Adv Radiat Oncol. 2019 Jul 30;5(1):1-16. doi: 10.1016/j.adro.2019.07.013. eCollection 2020 Jan-Feb. Adv Radiat Oncol. 2019. PMID: 32051885 Free PMC article. Review.
-
Image quality models for 2D and 3D x-ray imaging systems: A perspective vignette.Med Phys. 2023 Jun;50 Suppl 1:109-116. doi: 10.1002/mp.16051. Epub 2022 Dec 29. Med Phys. 2023. PMID: 36542332 Review.
Cited by
-
First implementation of an innovative infra-red camera system integrated into a mobile CBCT scanner for applicator tracking in brachytherapy-Initial performance characterization.J Appl Clin Med Phys. 2024 Jul;25(7):e14364. doi: 10.1002/acm2.14364. Epub 2024 Apr 16. J Appl Clin Med Phys. 2024. PMID: 38626753 Free PMC article.
-
Investigating the impact of breast positioning control on physical treatment parameters in multi-catheter breast brachytherapy.Strahlenther Onkol. 2024 Jan;200(1):49-59. doi: 10.1007/s00066-023-02127-0. Epub 2023 Aug 17. Strahlenther Onkol. 2024. PMID: 37676482 Free PMC article.
-
Narrowing the difference in dose delivery for IOERT and IOBT for locally advanced and locally recurrent rectal cancer.J Contemp Brachytherapy. 2022 Aug;14(4):370-378. doi: 10.5114/jcb.2022.118305. Epub 2022 Jul 21. J Contemp Brachytherapy. 2022. PMID: 36199944 Free PMC article.
-
Establishing an intraoperative, mobile CBCT-based workflow for gynecologic brachytherapy: primary experience and benefit assessment.Front Oncol. 2025 Apr 16;15:1562670. doi: 10.3389/fonc.2025.1562670. eCollection 2025. Front Oncol. 2025. PMID: 40308506 Free PMC article.
-
Is model-based dose calculation based on cone-beam computed tomography suitable for adaptive treatment planning in brachytherapy?Strahlenther Onkol. 2025 Jan;201(1):57-70. doi: 10.1007/s00066-024-02318-3. Epub 2024 Nov 27. Strahlenther Onkol. 2025. PMID: 39601857 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
