

Combining renal cell arrest and damage biomarkers to predict progressive AKI in patient with sepsis
- PMID: 34906098
- PMCID: PMC8672478
- DOI: 10.1186/s12882-021-02611-8
Combining renal cell arrest and damage biomarkers to predict progressive AKI in patient with sepsis
Abstract
Background: Sepsis is the most common trigger for AKI and up to 40% of mild or moderate septic AKI would progress to more severe AKI, which is associated with significantly increased risk for death and later CKD/ESRD. Early identifying high risk patients for AKI progression is a major challenge in patients with septic AKI.
Methods: This is a prospective, multicenter cohort study which enrolled adult patients with sepsis and initially developed stage 1 or 2 AKI in the intensive care unit from January 2014 to March 2018. AKI was diagnosed and staged according to 2012 KDIGO-AKI guidelines. Renal cell arrest biomarkers (urinary TIMP2*IGFBP7, u[TIMP-2]*[IGFBP7]) and renal damage biomarkers (urinary KIM-1[uKIM-1] and urinary IL-18 [uIL-18]) were measured at time of AKI clinical diagnosis, and the performance of biomarkers for predicting septic AKI progression alone or in combination were evaluated. The primary outcome was AKI progression defined as worsening of AKI stage. The secondary outcome was AKI progression with subsequent death during hospitalization.
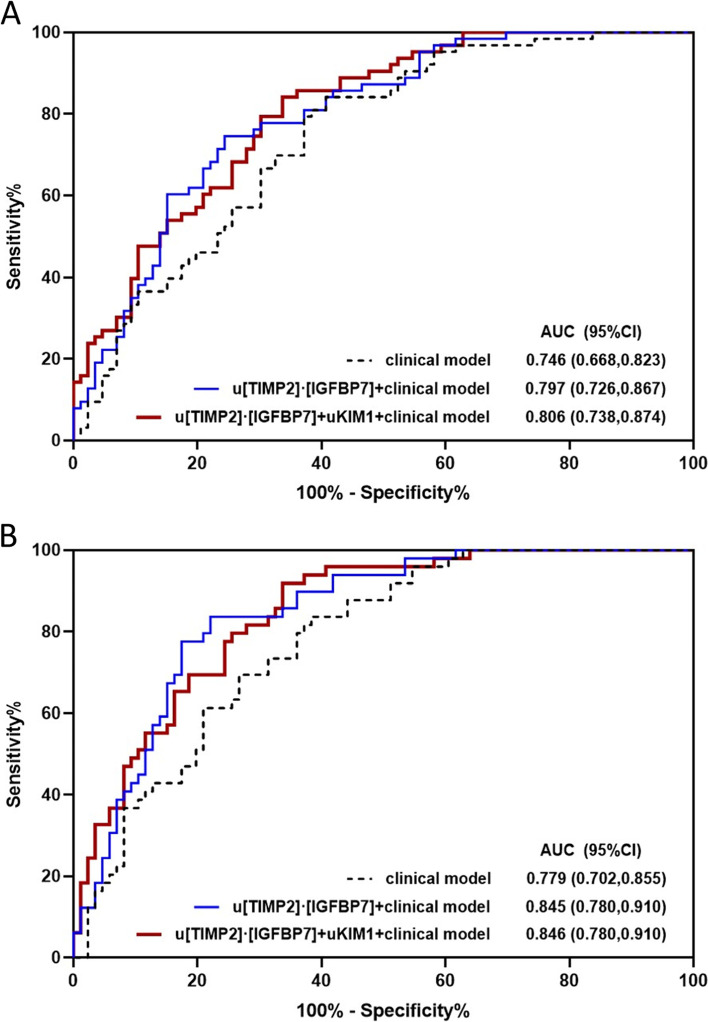
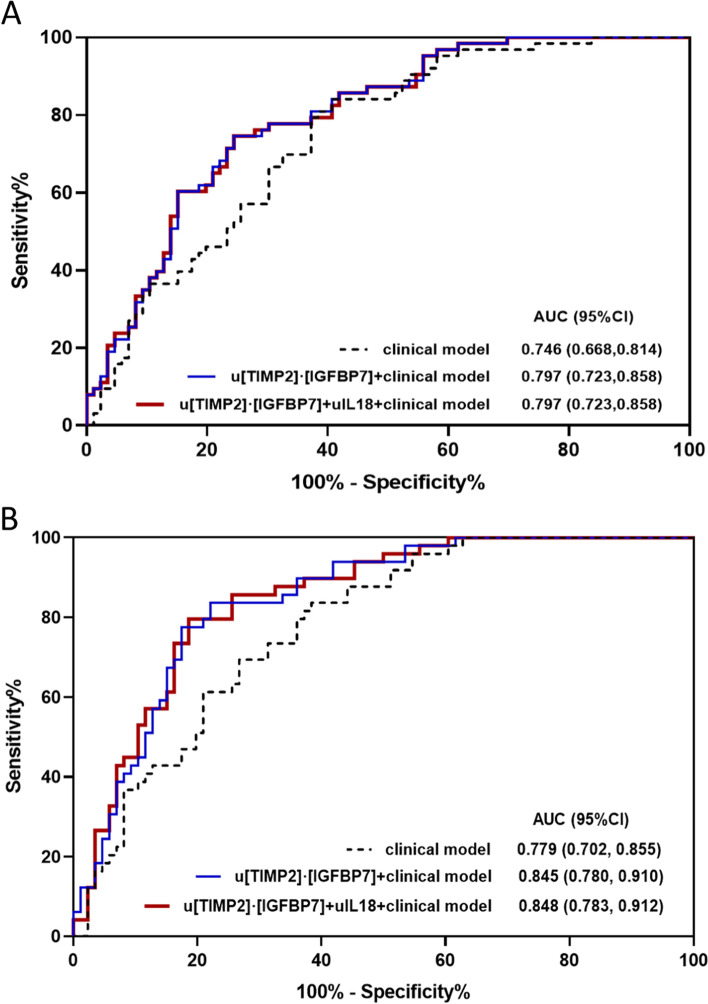
Results: Among 433 screened patients, 149 patients with sepsis and stage 1 or 2 AKI were included, in which 63 patients developed progressive AKI and 49 patients subsequently died during hospitalization. u[TIMP-2]*[IGFBP7], uKIM-1 and uIL-18 independently predicted the progression of septic AKI in which u[TIMP-2]*[IGFBP7] showed the greatest AUC (0.745; 95%CI, 0.667-0.823) as compared to uKIM-1 (AUC 0.719; 95%CI 0.638-0.800) and uIL-18 (AUC 0.619; 95%CI 0.525-0.731). Combination of u[TIMP-2]*[IGFBP7] with uKIM-1 improved the performance of predicting septic AKI progression with AUC of 0.752. u[TIMP-2]*[IGFBP7], alone or combined with uKIM-1/uIL-18, improved the risk reclassification over the clinical risk factor model alone both for the primary and secondary outcomes, as evidenced by significant category-free net reclassification index.
Conclusions: Combination of renal cell arrest and damage biomarkers enhanced the prediction of AKI progression in patients with sepsis and improved risk reclassification over the clinical risk factors.
Keywords: AKI; Biomarker; Progression; Risk prediction; Sepsis.
© 2021. The Author(s).
Conflict of interest statement
The authors have no conflict of interest to declare.
Figures
References
-
- Maizel J, Daubin D, Vong LV, Titeca-Beauport D, Wetzstein M, Kontar L, et al. Urinary TIMP2 and IGFBP7 identifies high risk patients of short-term progression from mild and moderate to severe acute kidney injury during septic shock: a prospective cohort study. Dis Markers. 2019;347:1215. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
