

Non-Invasive Approaches to Estimate Liver Steatosis and Stiffness in Children With Non-Alcoholic Fatty Liver Disease
- PMID: 34908012
- PMCID: PMC9673005
- DOI: 10.1097/MPG.0000000000003371
Non-Invasive Approaches to Estimate Liver Steatosis and Stiffness in Children With Non-Alcoholic Fatty Liver Disease
Abstract
Objectives: To develop pediatric-specific models that predict liver stiffness and hepatic steatosis in non-alcoholic fatty liver disease (NAFLD), based on clinical and laboratory data.
Methods: Children with NAFLD, who had undergone magnetic resonance imaging with proton density fat fraction (MRI-PDFF) for steatosis quantification and/or magnetic resonance elastography (MRE) for liver stiffness assessment were included. We used data from patients imaged between April 2009 to July 2018 to develop a predictive model for fat fraction and stiffness. We validated the performance of the models using data from a second cohort, imaged between 2018 and 2019.
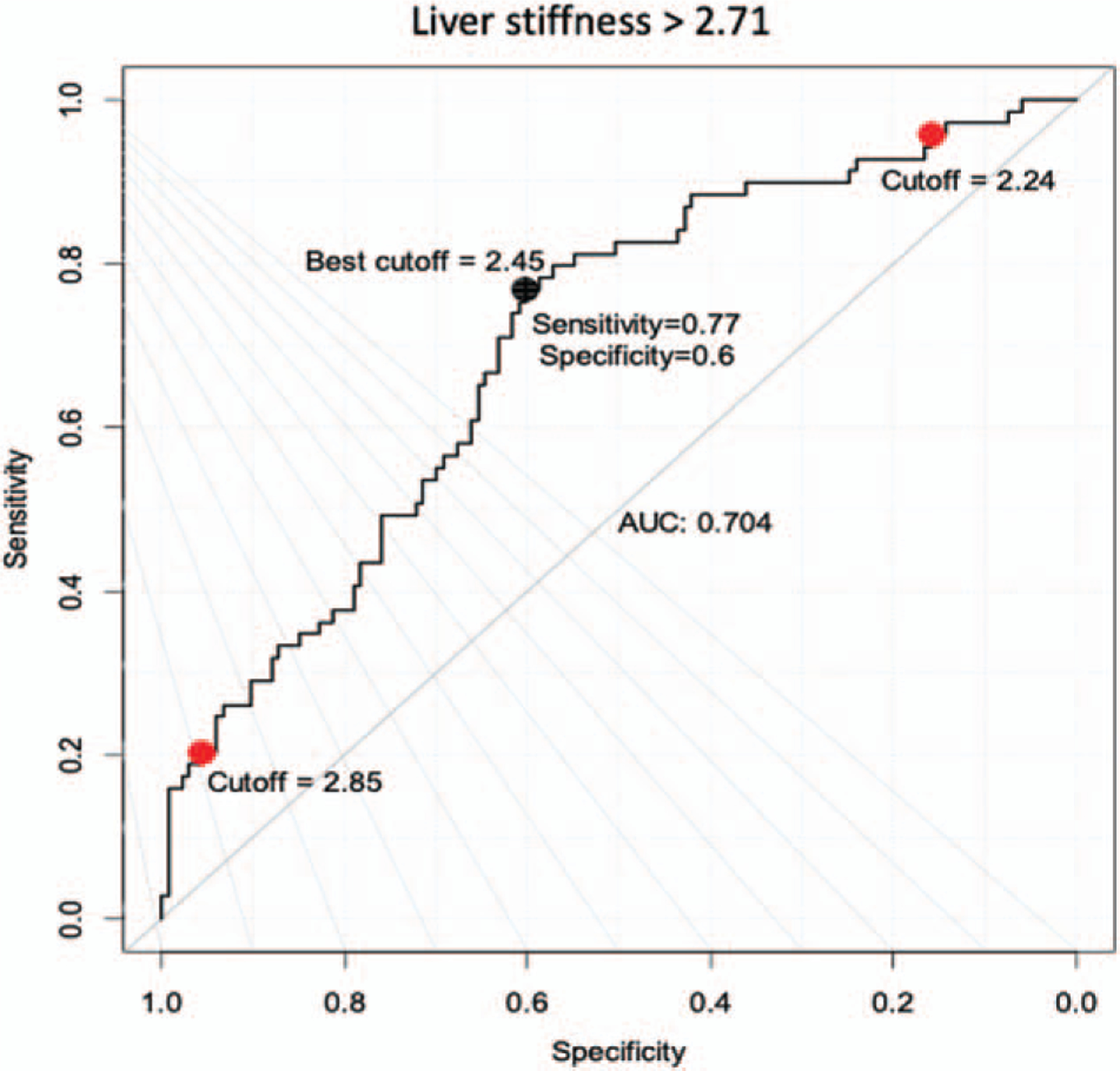
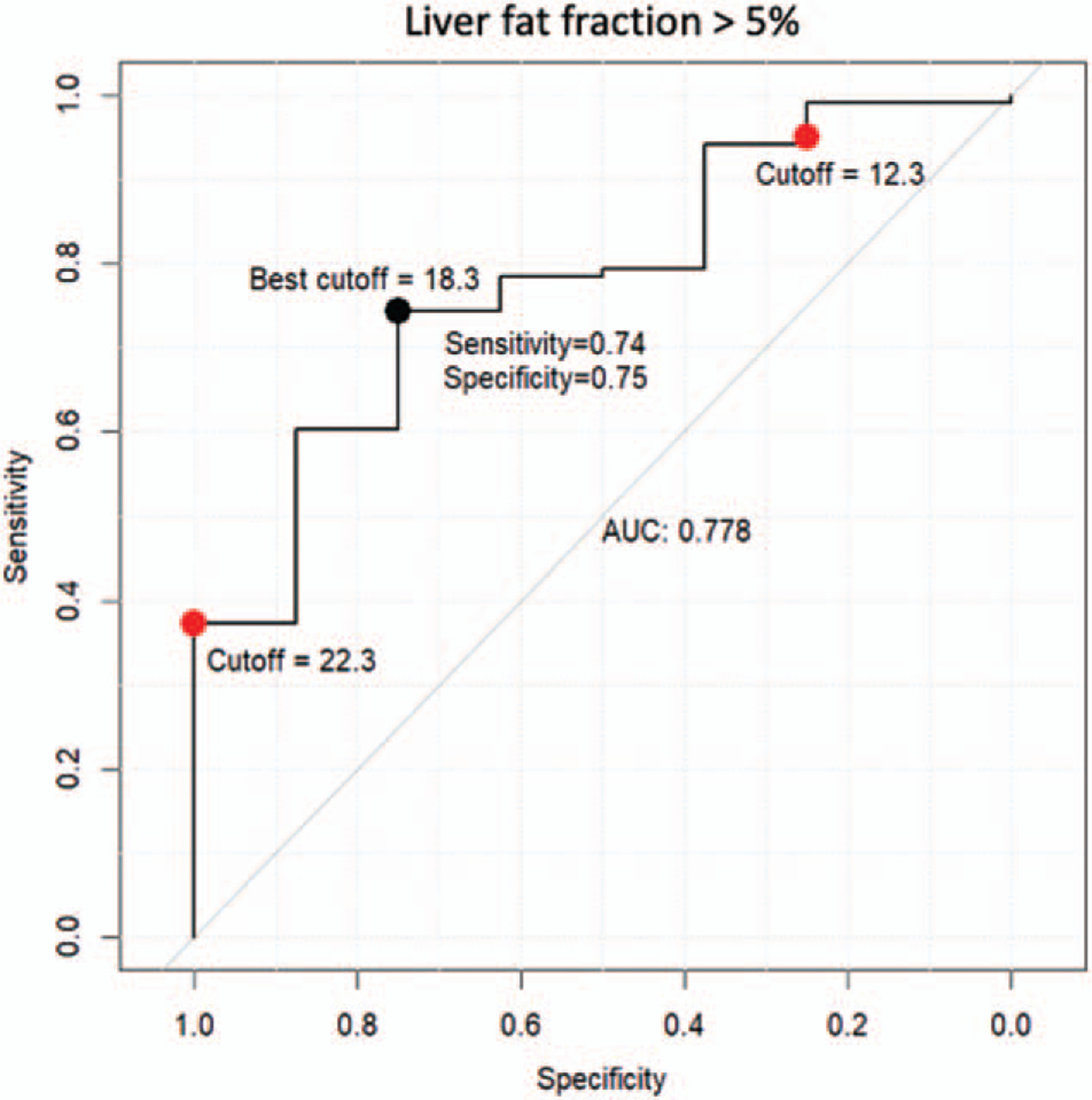
Results: The first cohort (n = 344) consisted of predominantly non-Hispanic (80%), male (67%) adolescents. MRE data were available for 343 children, while PDFF data were available for 130. In multivariable regression, ethnicity, insulin levels, platelet count, and aspartate aminotransferase independently predicted liver stiffness and these variables were used to develop the predictive model. Similarly, sex, ethnicity, alanine aminotransferase, and triglycerides levels independently predicted liver PDFF and were used in the PDFF model. The AUC of the optimal cutoff for the model that predicted a stiffness of >2.71 kPa was 0.70 and for the model that predicted PDFF >5% was 0.78. The validation group (n = 110) had similar characteristics. The correlation coefficient of the model with the measured liver stiffness was 0.30 and with the measured liver PDFF was 0.26.
Conclusions: Pediatric-specific models perform poorly at predicting exact liver stiffness and steatosis; however, in the absence of magnetic resonance imaging can be used to predict the presence of significant steatosis (>5%) and/or significant stiffness (>2.71). Thus, imaging remains an invaluable adjunct to laboratory investigations in determining disease severity.
Copyright © 2021 by European Society for Pediatric Gastroenterology, Hepatology, and Nutrition and North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Dhaliwal J, Chavhan GB, Lurz E, et al. Hepatic steatosis is highly prevalent across the paediatric age spectrum, including in pre-school age children. Aliment Pharmacol Ther 2018;48:556–63. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
