

Reinterventions after damage control surgery
- PMID: 34908623
- PMCID: PMC8634277
- DOI: 10.25100/cm.v52i2.4805
Reinterventions after damage control surgery
Abstract
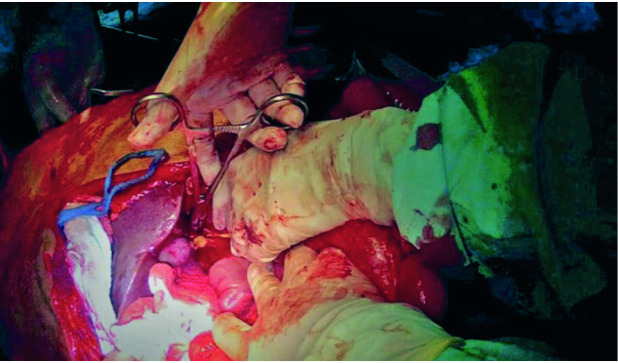
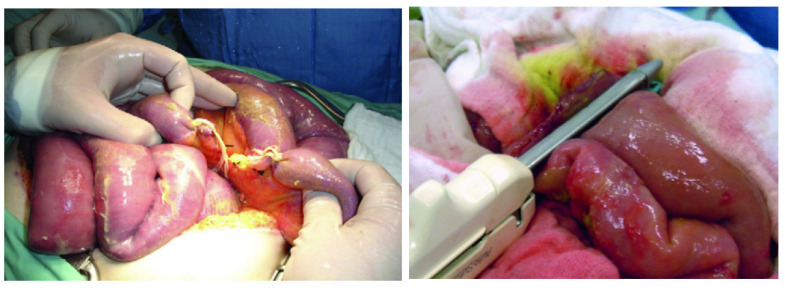
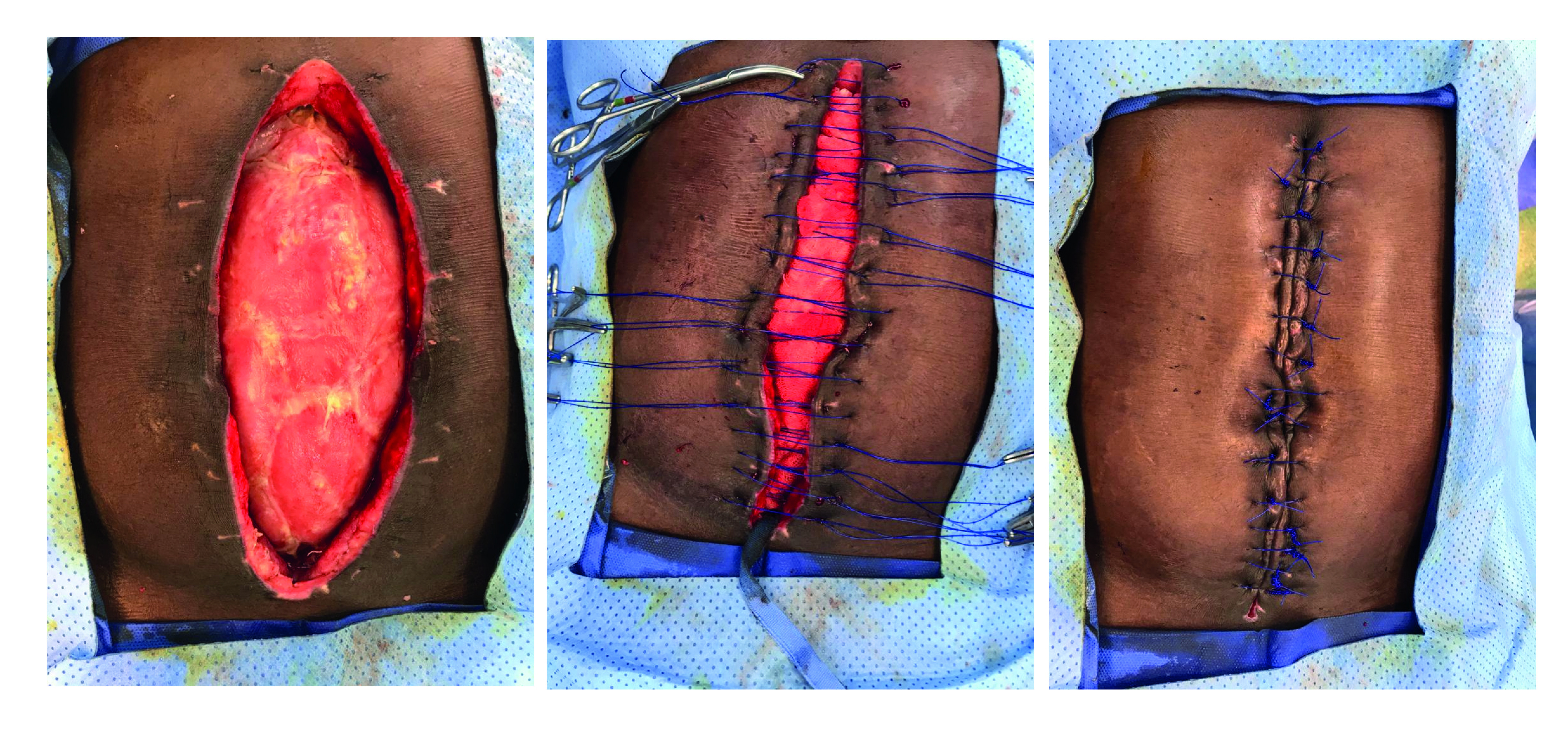
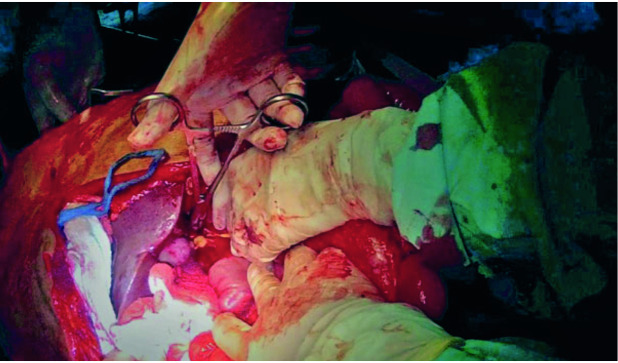
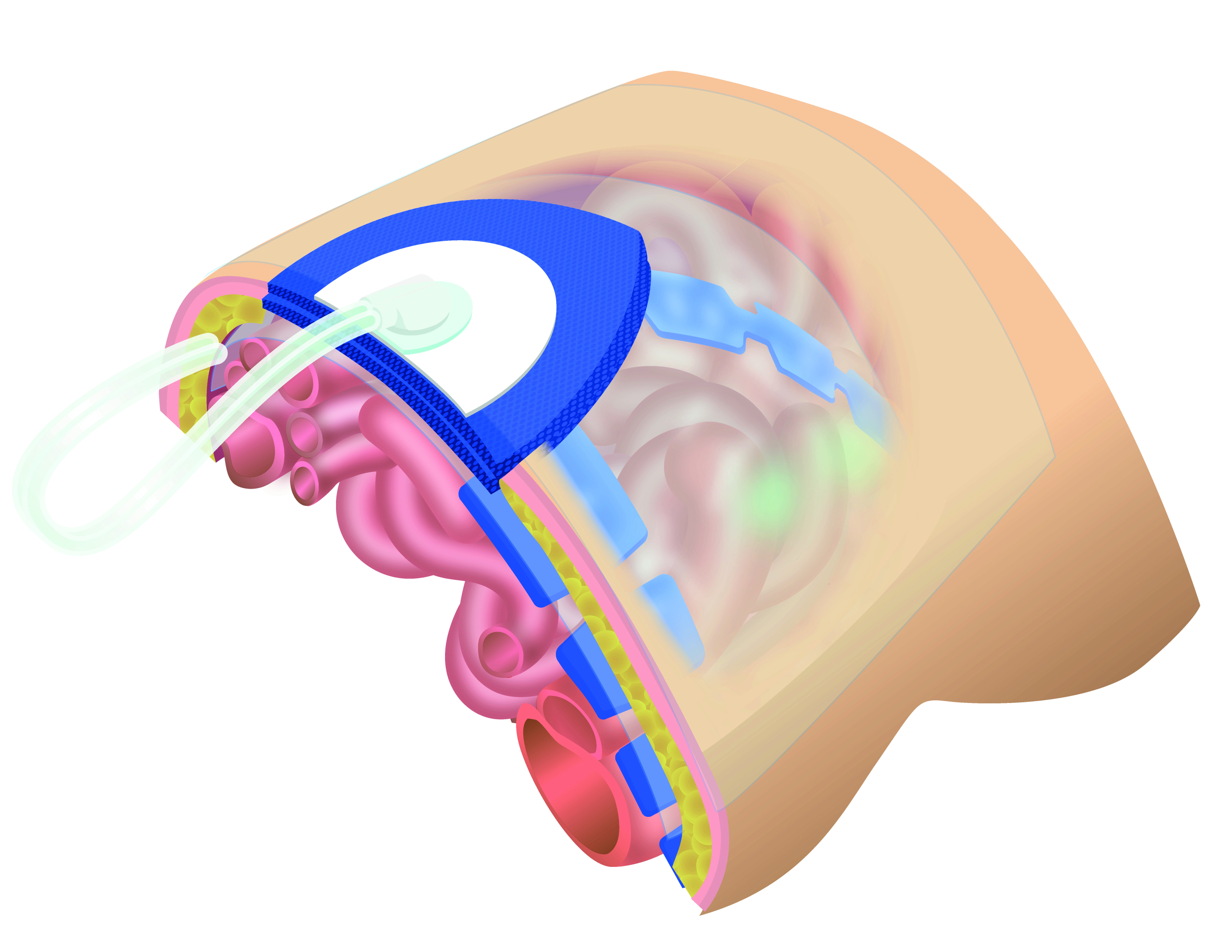
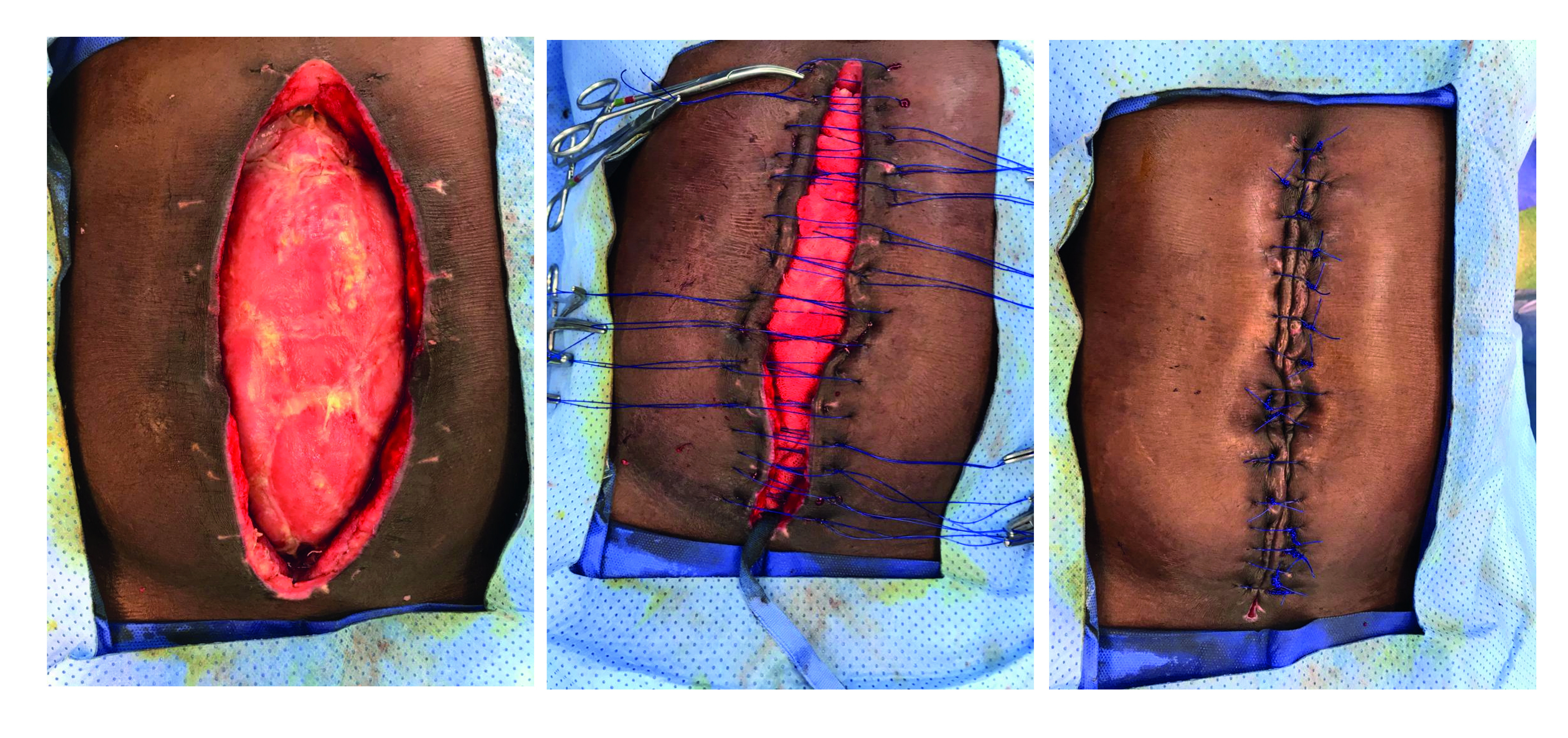
Damage control has well-defined steps. However, there are still controversies regarding whom, when, and how re-interventions should be performed. This article summarizes the Trauma and Emergency Surgery Group (CTE) Cali-Colombia recommendations about the specific situations concerning second interventions of patients undergoing damage control surgery. We suggest packing as the preferred bleeding control strategy, followed by unpacking within the next 48-72 hours. In addition, a deferred anastomosis is recommended for correction of intestinal lesions, and patients treated with vascular shunts should be re-intervened within 24 hours for definitive management. Furthermore, abdominal or thoracic wall closure should be attempted within eight days. These strategies aim to decrease complications, morbidity, and mortality.
El control de daños es uno de los pilares de la cirugía de trauma. Sin embargo, la reintervención aún genera controversias en cuanto a quién, cuándo y cómo debe realizarse. El presente artículo presenta las recomendaciones del grupo de Cirugía de Trauma y Emergencias (CTE) de Cali, Colombia, respecto a las reintervenciones después de una cirugía de control de daños. Se recomienda el empaquetamiento como la estrategia de control de sangrado y se debe desempaquetar en un lapso entre 48 y 72 horas. La anastomosis diferida debe ser la opción de reparo en las lesiones intestinales. La reintervención vascular en los pacientes manejados con shunt vascular debe ser antes de las 24 horas para dar el manejo definitivo. En un lapso de 8 días se debe intentar realizar el cierre de la pared abdominal o torácica. Estas estrategias buscan disminuir la frecuencia de complicaciones y de morbimortalidad.
Keywords: Laparotomy; abdominal wall; anastomosis surgical; cardiac surgical procedures; colostomy; intensive care units; intra-abdominal hypertension; ostomy; postoperative period; reoperation; surgical wound infection; thoracic cavity.
Copyright © 2021 Colombia Medica.
Conflict of interest statement
Conflict of interest: The authors declare that they have no conflict of interest.
Figures




References
-
- Rotondo MF, Schwab CW, McGonigal MD, Phillips GR, Fruchterman TM, Kauder DR. et al "Damage control": an approach for improved survival in exsanguinating penetrating abdominal injury Trauma. 1993;35:375–382. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
