

Fractures of the femoral head: a narrative review
- PMID: 34909230
- PMCID: PMC8631236
- DOI: 10.1302/2058-5241.6.210034
Fractures of the femoral head: a narrative review
Abstract
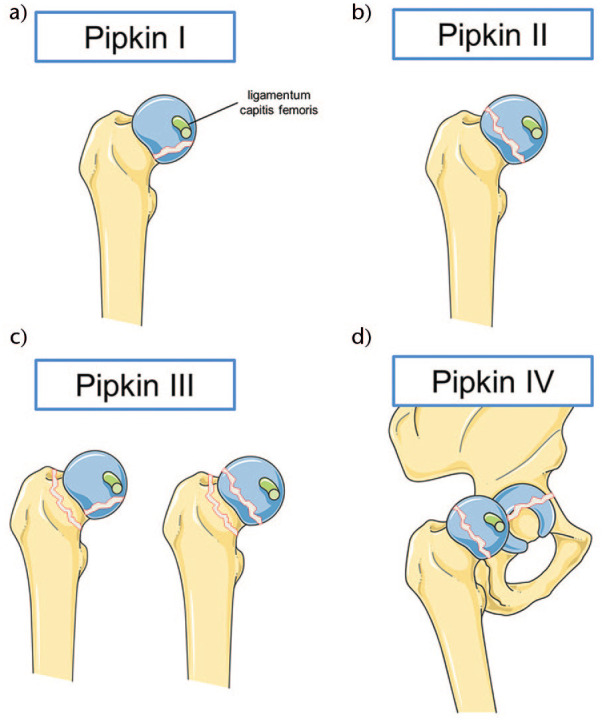
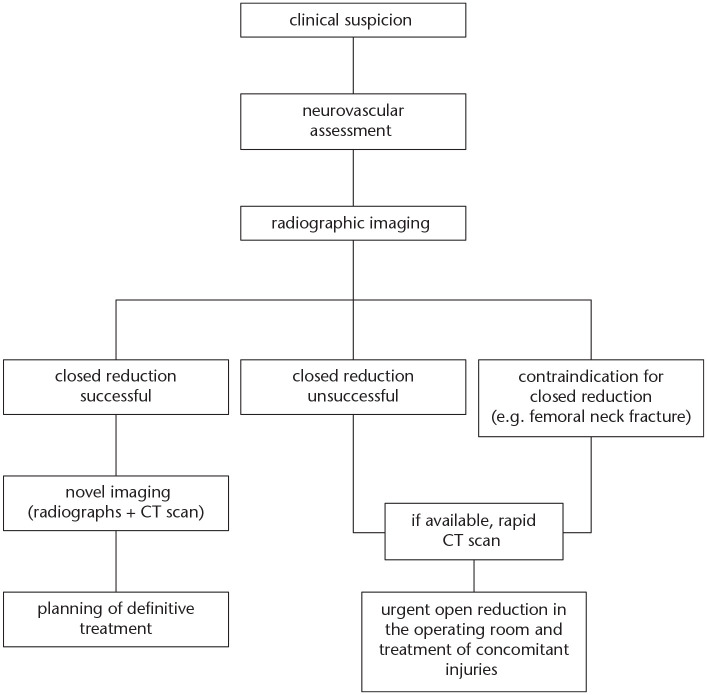
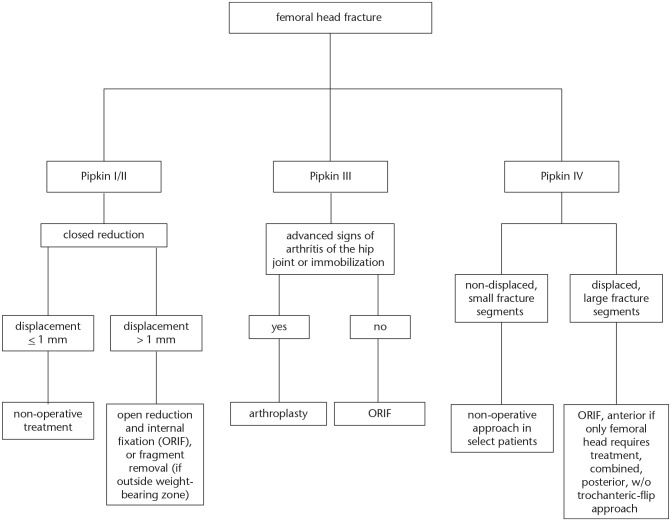
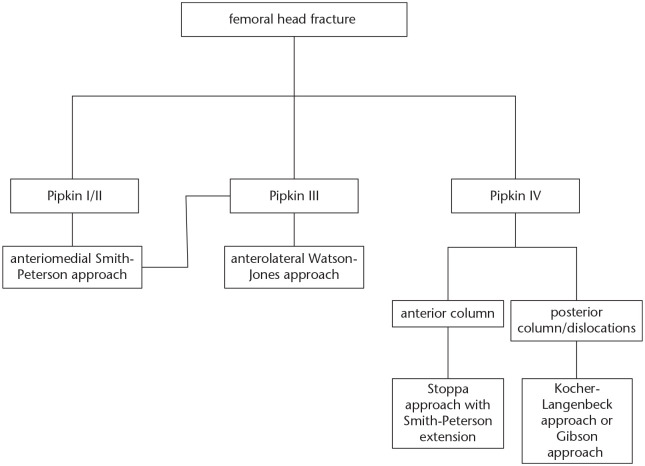
Fractures of the femoral head are rare injuries, which typically occur after posterior hip dislocation.The Pipkin classification, developed in 1957, is the most commonly used classification scheme to date.The injury is mostly caused by high-energy trauma, such as motor vehicle accidents or falls from a significant height.Emergency treatment consists of urgent closed reduction of the hip joint, followed by non-operative or operative treatment of the femoral head fracture and any associated injuries.There is an ongoing controversy about the suitable surgical approach (anterior vs. posterior) for addressing fractures of the femoral head. Fracture location, degree of displacement, joint congruity and the presence of loose fragments, as well as concomitant injuries are crucial factors in choosing the adequate surgical approach.Long-term complications such as osteonecrosis of the femoral head, posttraumatic osteoarthritis and heterotopic ossification can lead to a relatively poor functional outcome. Cite this article: EFORT Open Rev 2021;6:1122-1131. DOI: 10.1302/2058-5241.6.210034.
Keywords: Pipkin; classification; femoral head; fracture; surgical approach.
© 2021 The author(s).
Conflict of interest statement
ICMJE Conflict of interest statement: The authors declare no conflict of interest relevant to this work.
Figures
References
-
- Hougaard K, Thomsen PB. Traumatic posterior fracture-dislocation of the hip with fracture of the femoral head or neck, or both. J Bone Joint Surg [Am] 1988;70-A:233–239. - PubMed
-
- Roeder LF, Jr, DeLee JC. Femoral head fractures associated with posterior hip dislocation. Clin Orthop Relat Res 1980;147:121–130. - PubMed
-
- Epstein HC, Wiss DA, Cozen L. Posterior fracture dislocation of the hip with fractures of the femoral head. Clin Orthop Relat Res 1985;201:9–17. - PubMed
-
- Birkett J. Description of a dislocation of the head of the femur, complicated with its fracture; with remarks. 1869. Clin Orthop Relat Res 2007;458:10–11. - PubMed
-
- Droll KP, Broekhuyse H, O’Brien P. Fracture of the femoral head. J Am Acad Orthop Surg 2007;15:716–727. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
