

This is a preprint.
SARS-CoV-2 incidence, transmission and reinfection in a rural and an urban setting: results of the PHIRST-C cohort study, South Africa, 2020-2021
- PMID: 34909794
- PMCID: PMC8669861
- DOI: 10.1101/2021.07.20.21260855
SARS-CoV-2 incidence, transmission and reinfection in a rural and an urban setting: results of the PHIRST-C cohort study, South Africa, 2020-2021
Update in
-
SARS-CoV-2 incidence, transmission, and reinfection in a rural and an urban setting: results of the PHIRST-C cohort study, South Africa, 2020-21.Lancet Infect Dis. 2022 Jun;22(6):821-834. doi: 10.1016/S1473-3099(22)00069-X. Epub 2022 Mar 14. Lancet Infect Dis. 2022. PMID: 35298900 Free PMC article.
Abstract
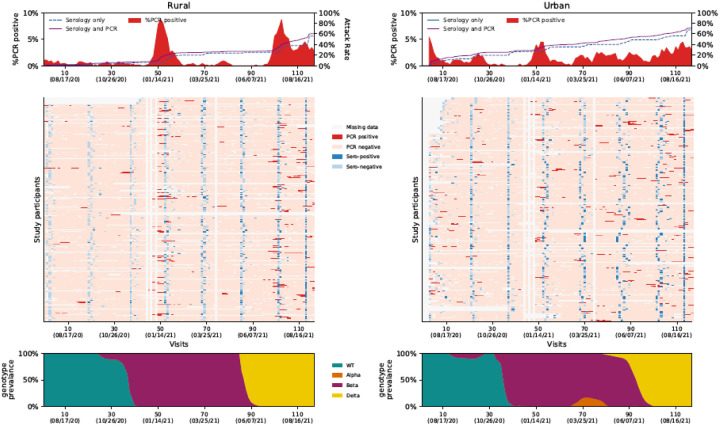
Background: By August 2021, South Africa experienced three SARS-CoV-2 waves; the second and third associated with emergence of Beta and Delta variants respectively.
Methods: We conducted a prospective cohort study during July 2020-August 2021 in one rural and one urban community. Mid-turbinate nasal swabs were collected twice-weekly from household members irrespective of symptoms and tested for SARS-CoV-2 using real-time reverse transcription polymerase chain reaction (rRT-PCR). Serum was collected every two months and tested for anti-SARS-CoV-2 antibodies.
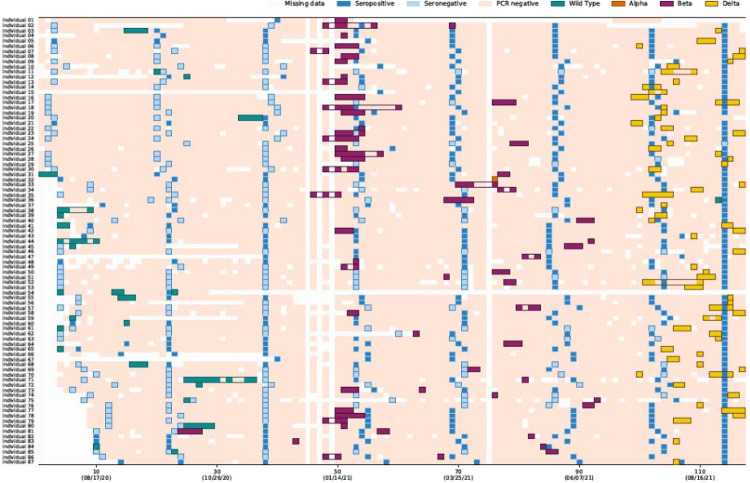
Results: Among 115,759 nasal specimens from 1,200 members (follow-up rate 93%), 1976 (2%) were SARS-CoV-2-positive. By rRT-PCR and serology combined, 62% (749/1200) of individuals experienced ≥1 SARS-CoV-2 infection episode, and 12% (87/749) experienced reinfection. Of 662 PCR-confirmed episodes with available data, 15% (n=97) were associated with ≥1 symptom. Among 222 households, 200 (90%) had ≥1 SARS-CoV-2-positive individual. Household cumulative infection risk (HCIR) was 25% (213/856). On multivariable analysis, accounting for age and sex, index case lower cycle threshold value (OR 3.9, 95%CI 1.7-8.8), urban community (OR 2.0,95%CI 1.1-3.9), Beta (OR 4.2, 95%CI 1.7-10.1) and Delta (OR 14.6, 95%CI 5.7-37.5) variant infection were associated with increased HCIR. HCIR was similar for symptomatic (21/110, 19%) and asymptomatic (195/775, 25%) index cases (p=0.165). Attack rates were highest in individuals aged 13-18 years and individuals in this age group were more likely to experience repeat infections and to acquire SARS-CoV-2 infection. People living with HIV who were not virally supressed were more likely to develop symptomatic illness, and shed SARS-CoV-2 for longer compared to HIV-uninfected individuals.
Conclusions: In this study, 85% of SARS-CoV-2 infections were asymptomatic and index case symptom status did not affect HCIR, suggesting a limited role for control measures targeting symptomatic individuals. Increased household transmission of Beta and Delta variants, likely contributed to successive waves, with >60% of individuals infected by the end of follow-up.
Research in context: Evidence before this study: Previous studies have generated wide-ranging estimates of the proportion of SARS-CoV-2 infections which are asymptomatic. A recent systematic review found that 20% (95% CI 3%-67%) of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infections remained asymptomatic throughout infection and that transmission from asymptomatic individuals was reduced. A systematic review and meta-analysis of 87 household transmission studies of SARS-CoV-2 found an estimated secondary attack rate of 19% (95% CI 16-22). The review also found that household secondary attack rates were increased from symptomatic index cases and that adults were more likely to acquire infection. As of December 2021, South Africa experienced three waves of SARS-CoV-2 infections; the second and third waves were associated with circulation of Beta and Delta variants respectively. SARS-CoV-2 vaccines became available in February 2021, but uptake was low in study sites reaching 5% fully vaccinated at the end of follow up. Studies to quantify the burden of asymptomatic infections, symptomatic fraction, reinfection frequency, duration of shedding and household transmission of SARS-CoV-2 from asymptomatically infected individuals have mostly been conducted as part of outbreak investigations or in specific settings. Comprehensive systematic community studies of SARS-CoV-2 burden and transmission including for the Beta and Delta variants are lacking, especially in low vaccination settings.Added value of this study: We conducted a unique detailed COVID-19 household cohort study over a 13 month period in South Africa, with real time reverse transcriptase polymerase chain reaction (rRT-PCR) testing twice a week irrespective of symptoms and bimonthly serology. By the end of the study in August 2021, 749 (62%) of 1200 individuals from 222 randomly sampled households in a rural and an urban community in South Africa had at least one confirmed SARS-CoV-2 infection, detected on rRT-PCR and/or serology, and 12% (87/749) experienced reinfection. Symptom data were analysed for 662 rRT-PCR-confirmed infection episodes that occurred >14 days after the start of follow-up (of a total of 718 rRT-PCR-confirmed episodes), of these, 15% (n=97) were associated with one or more symptoms. Among symptomatic indvidiausl, 9% (n=9) were hospitalised and 2% (n=2) died. Ninety percent (200/222) of included households, had one or more individual infected with SARS-CoV-2 on rRT-PCR and/or serology within the household. SARS-CoV-2 infected index cases transmitted the infection to 25% (213/856) of susceptible household contacts. Index case ribonucleic acid (RNA) viral load proxied by rRT-PCR cycle threshold value was strongly predictive of household transmission. Presence of symptoms in the index case was not associated with household transmission. Household transmission was four times greater from index cases infected with Beta variant and fifteen times greater from index cases infected with Delta variant compared to wild-type infection. Attack rates were highest in individuals aged 13-18 years and individuals in this age group were more likely to experience repeat infections and to acquire SARS-CoV-2 infection within households. People living with HIV (PLHIV) who were not virally supressed were more likely to develop symptomatic illness when infected with SARS-CoV-2, and shed SARS-CoV-2 for longer when compared to HIV-uninfected individuals.Implications of all the available evidence: We found a high rate of SARS-CoV-2 infection in households in a rural community and an urban community in South Africa, with the majority of infections being asymptomatic in individuals of all ages. Asymptomatic individuals transmitted SARS-CoV-2 at similar levels to symptomatic individuals suggesting that interventions targeting symptomatic individuals such as symptom-based testing and contact tracing of individuals tested because they report symptoms may have a limited impact as control measures. Increased household transmission of Beta and Delta variants, likely contributed to recurrent waves of COVID-19, with >60% of individuals infected by the end of follow-up. Higher attack rates, reinfection and acquisition in adolescents and prolonged SARS-CoV-2 shedding in PLHIV who were not virally suppressed suggests that prioritised vaccination of individuals in these groups could impact community transmission.
Figures
Similar articles
-
SARS-CoV-2 incidence, transmission, and reinfection in a rural and an urban setting: results of the PHIRST-C cohort study, South Africa, 2020-21.Lancet Infect Dis. 2022 Jun;22(6):821-834. doi: 10.1016/S1473-3099(22)00069-X. Epub 2022 Mar 14. Lancet Infect Dis. 2022. PMID: 35298900 Free PMC article.
-
Characteristics of infections with ancestral, Beta and Delta variants of SARS-CoV-2 in the PHIRST-C community cohort study, South Africa, 2020-2021.BMC Infect Dis. 2024 Mar 21;24(1):336. doi: 10.1186/s12879-024-09209-z. BMC Infect Dis. 2024. PMID: 38515050 Free PMC article.
-
Asymptomatic transmission and high community burden of seasonal influenza in an urban and a rural community in South Africa, 2017-18 (PHIRST): a population cohort study.Lancet Glob Health. 2021 Jun;9(6):e863-e874. doi: 10.1016/S2214-109X(21)00141-8. Lancet Glob Health. 2021. PMID: 34019838 Free PMC article.
-
Universal screening for SARS-CoV-2 infection: a rapid review.Cochrane Database Syst Rev. 2020 Sep 15;9(9):CD013718. doi: 10.1002/14651858.CD013718. Cochrane Database Syst Rev. 2020. PMID: 33502003 Free PMC article.
-
Household Transmission of SARS-CoV-2: A Systematic Review and Meta-analysis.JAMA Netw Open. 2020 Dec 1;3(12):e2031756. doi: 10.1001/jamanetworkopen.2020.31756. JAMA Netw Open. 2020. PMID: 33315116 Free PMC article.
Cited by
-
Impact of HIV on COVID-19 Outcomes: A Propensity Score Matching Analysis with Varying Age Differences.AIDS Behav. 2024 Oct;28(Suppl 1):124-135. doi: 10.1007/s10461-023-04088-y. Epub 2023 Jun 8. AIDS Behav. 2024. PMID: 37289345 Free PMC article.
-
Associations of County-Level Social Determinants of Health with COVID-19 Related Hospitalization Among People with HIV: A Retrospective Analysis of the U.S. National COVID Cohort Collaborative (N3C).AIDS Behav. 2024 Oct;28(Suppl 1):136-148. doi: 10.1007/s10461-024-04466-0. Epub 2024 Sep 18. AIDS Behav. 2024. PMID: 39292319 Free PMC article.
-
Scoping review: longitudinal effects of the COVID-19 pandemic on child and adolescent mental health.Eur Child Adolesc Psychiatry. 2024 May;33(5):1257-1312. doi: 10.1007/s00787-023-02206-8. Epub 2023 Apr 21. Eur Child Adolesc Psychiatry. 2024. PMID: 37081139 Free PMC article.
References
-
- Hsiao M, Davies MA, Kalk E, et al. SARS-COV-2 SEROPREVALENCE IN THE CAPE TOWN METROPOLITAN SUB-DISTRICTS AFTER THE PEAK OF INFECTIONS. NICD Public Heal Surveill Bull. 2020;18(Supplementary Issue 5):2–9.
-
- Statistics South Africa, StatsSA. Statistical Release P0302: Mid-year population estimates 2020. Stats SA. 2020;(July):1–22. http://www.statssa.gov.za/publications/P0302/P03022017.pdf.
-
- Simbayi L, Zuma K, Zungu N, et al. South African National HIV Prevalence, Incidence, Behaviour and Communication Survey, 2017. Cape Town, South Africa; 2017.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous