

Outcomes of a Delirium Prevention Program in Older Persons After Elective Surgery: A Stepped-Wedge Cluster Randomized Clinical Trial
- PMID: 34910080
- PMCID: PMC8674802
- DOI: 10.1001/jamasurg.2021.6370
Outcomes of a Delirium Prevention Program in Older Persons After Elective Surgery: A Stepped-Wedge Cluster Randomized Clinical Trial
Abstract
Importance: Delirium significantly worsens elective surgery outcomes and costs. Delirium risk is highest in elderly populations, whose surgical health care resource consumption (50%) exceeds their demographic proportion (15% to 18%) in high-resource countries. Effective nonpharmacologic delirium prevention could safely improve care in these vulnerable patients, but data from procedure-specific studies are insufficiently compelling to drive changes in practice. Delirium prevention approaches applicable to different surgical settings remain unexplored.
Objective: To examine whether a multifaceted prevention intervention is effective in reducing postoperative delirium incidence and prevalence after various major surgical procedures.
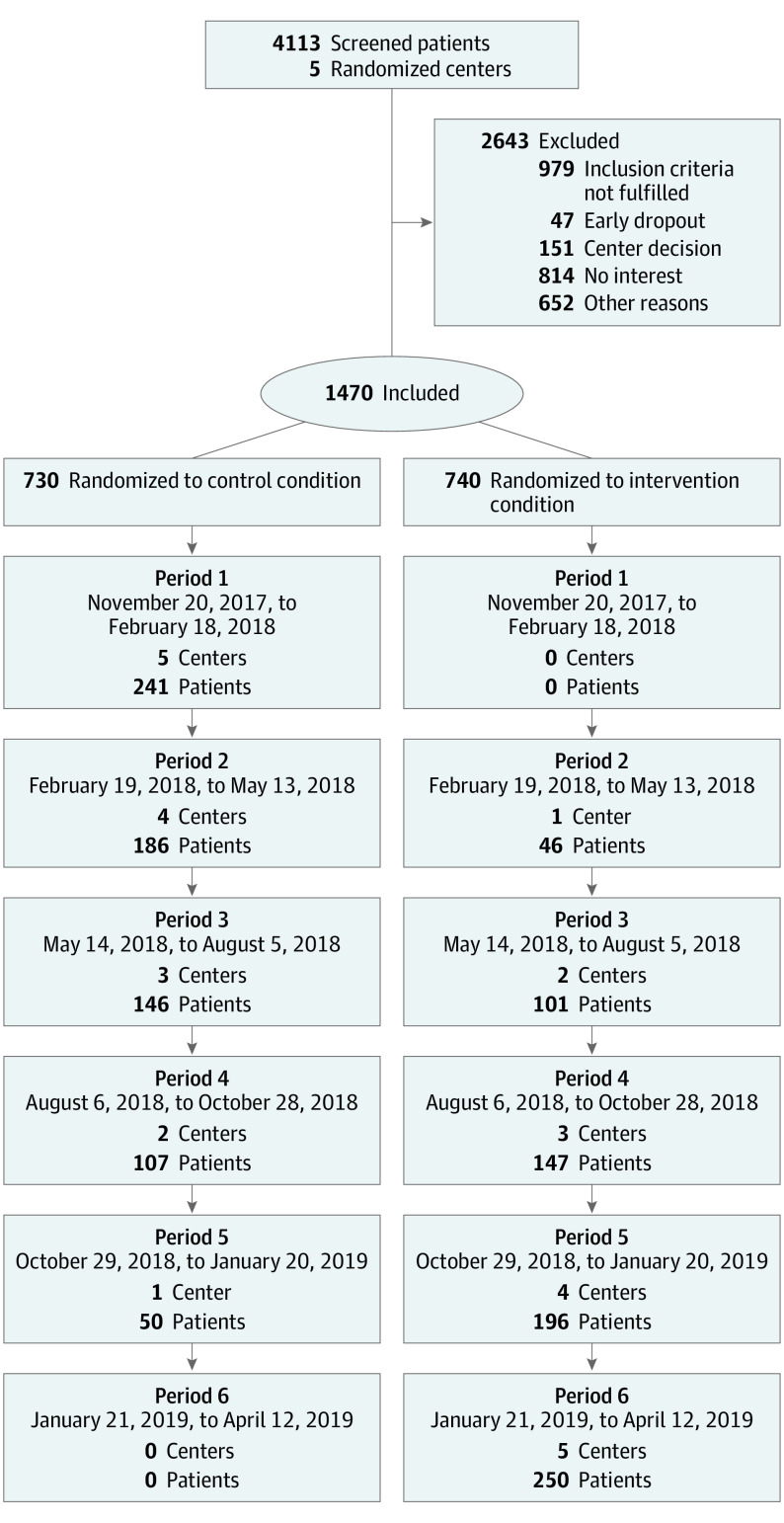
Design, setting, and participants: This stepped-wedge cluster randomized trial recruited 1470 patients 70 years and older undergoing elective orthopedic, general, or cardiac surgery from November 2017 to April 2019 from 5 German tertiary medical centers. Data were analyzed from December 2019 to July 2021.
Interventions: First, structured delirium education was provided to clinical caregivers at each site. Then, the study delirium prevention team assessed patient delirium risk factors and symptoms daily. Prevention was tailored to individual patient needs and could include: cognitive, motor, and sensory stimulation; meal companionship; accompaniment during diagnostic procedures; stress relaxation; and sleep promotion.
Main outcomes and measures: Postoperative delirium incidence and duration.
Results: Of 1470 included patients, 763 (51.9%) were male, and the median (IQR) age was 77 (74-81) years. Overall, the intervention reduced postoperative delirium incidence (odds ratio, 0.87; 95% CI, 0.77-0.98; P = .02) and percentage of days with delirium (intervention, 5.3%; control, 6.9%; P = .03). The effect was significant in patients undergoing orthopedic or abdominal surgery (odds ratio, 0.59; 95% CI, 0.35-0.99; P = .047) but not cardiac surgery (odds ratio, 1.18; 95% CI, 0.70-1.99; P = .54).
Conclusions and relevance: This multifaceted multidisciplinary prevention intervention reduced postoperative delirium occurrence and days with delirium in older patients undergoing different elective surgical procedures but not cardiac procedures. These results suggest implementing this delirium prevention program will improve care and outcomes in older patients undergoing elective general and orthopedic procedures.
Conflict of interest statement
References
-
- Scottish Intercollegiate Guidelines Network . Risk reduction and management of delirium. Accessed October 6, 2021. https://www.sign.ac.uk/sign-157-delirium - PubMed
-
- Australian Commission on Safety and Quality in Health Care . Delirium clinical care standard. Accessed October 6, 2021. https://www.safetyandquality.gov.au/our-work/clinical-care-standards/del...
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
