

Histopathological Evaluation of Deceased Persons in Lusaka, Zambia With or Without Coronavirus Disease 2019 (COVID-19) Infection: Results Obtained From Minimally Invasive Tissue Sampling
- PMID: 34910177
- PMCID: PMC8672753
- DOI: 10.1093/cid/ciab858
Histopathological Evaluation of Deceased Persons in Lusaka, Zambia With or Without Coronavirus Disease 2019 (COVID-19) Infection: Results Obtained From Minimally Invasive Tissue Sampling
Abstract
Background: Although much has been learned about the pathophysiology of coronavirus disease 2019 (COVID-19) infections, pathology data from patients who have died of COVID-19 in low- and middle-income country settings remain sparse. We integrated minimally invasive tissue sampling (MITS) into an ongoing postmortem surveillance study of COVID-19 in deceased individuals of all ages in Lusaka, Zambia.
Methods: We enrolled deceased subjects from the University Teaching Hospital Morgue in Lusaka, Zambia within 48 hours of death. We collected clinical and demographic information, a nasopharyngeal swab, and core tissue biopsies from the lung, liver, and kidneys for pathologic analysis. Individuals were considered eligible for MITS if they had a respiratory syndrome prior to death or a COVID-19+ polymerase chain reaction (PCR) nasopharyngeal swab specimen. Samples were retested using quantitative reverse transcriptase PCR.
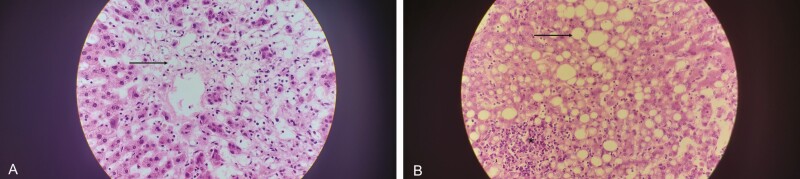
Results: From June to September 2020 we performed MITS on 29 deceased individuals. PCR results were available for 28/29 (96.5%) cases. Three had a COVID-19+ diagnosis antemortem, and 5 more were identified postmortem using the recommended cycle threshold cut-point <40. When expanding the PCR threshold to 40 ≤ cycle threshold (Ct) ≤ 45, we identified 1 additional case. Most cases were male and occurred in the community The median age at death was 47 years (range 40-64). Human immunodeficiency virus (HIV)/AIDS, tuberculosis, and diabetes were more common among the COVID-19+ cases. Diffuse alveolar damage and interstitial pneumonitis were common among COVID-19+ cases; nonspecific findings of hepatic steatosis and acute kidney injury were also prevalent in the COVID-19+ group. Vascular thrombi were rarely detected.
Conclusions: Lung abnormalities typical of viral pneumonias were common among deceased COVID-19+ individuals, as were nonspecific findings in the liver and kidneys. Pulmonary vascular thrombi were rarely detected, which could be a limitation of the MITS technique. Nonetheless, MITS offers a valuable alternative to open autopsy for understanding pathological changes due to COVID-19.
Keywords: COVID-19; autopsy; minimally invasive tissue sampling; pathology; postmortem.
© The Author(s) 2021. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures




References
-
- World Health Organization. WHO COVID-19 dashboard. Available at: https://covid19.who.int/.
-
- Zambia National Public Health Institute. Zambia COVID-19 situation report no. 161. Lusaka: National Public Health Institute, 2021.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
