

Diagnosing capillary leak in critically ill patients: development of an innovative scoring instrument for non-invasive detection
- PMID: 34910264
- PMCID: PMC8674404
- DOI: 10.1186/s13613-021-00965-8
Diagnosing capillary leak in critically ill patients: development of an innovative scoring instrument for non-invasive detection
Abstract
Background: The concomitant occurrence of the symptoms intravascular hypovolemia, peripheral edema and hemodynamic instability is typically named Capillary Leak Syndrome (CLS) and often occurs in surgical critical ill patients. However, neither a unitary definition nor standardized diagnostic criteria exist so far. We aimed to investigate common characteristics of this phenomenon with a subsequent scoring system, determining whether CLS contributes to mortality.
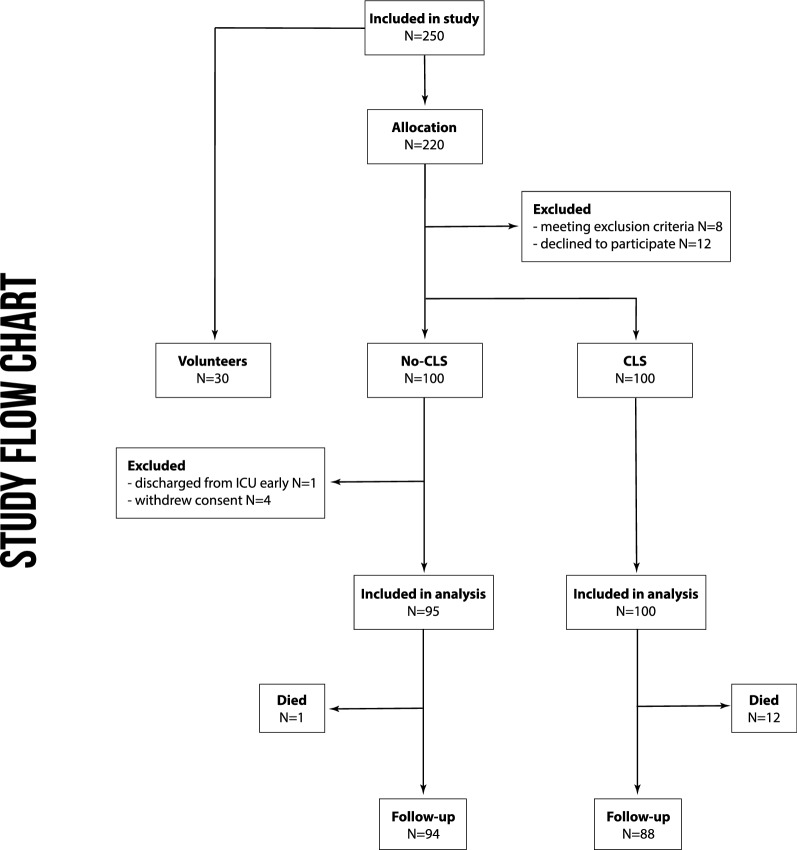
Methods: We conducted this single-center, observational, multidisciplinary, prospective trial in two separately run surgical ICUs of a tertiary academic medical center. 200 surgical patients admitted to the ICU and 30 healthy volunteers were included. Patients were clinically diagnosed as CLS or No-CLS group (each N = 100) according to the grade of edema, intravascular hypovolemia, hemodynamic instability, and positive fluid balance by two independent attending physicians with > 10 years of experience in ICU. We performed daily measurements with non-invasive body impedance electrical analysis, ultrasound and analysis of serum biomarkers to generate objective diagnostic criteria. Receiver operating characteristics were used, while we developed machine learning models to increase diagnostic specifications for our scoring model.
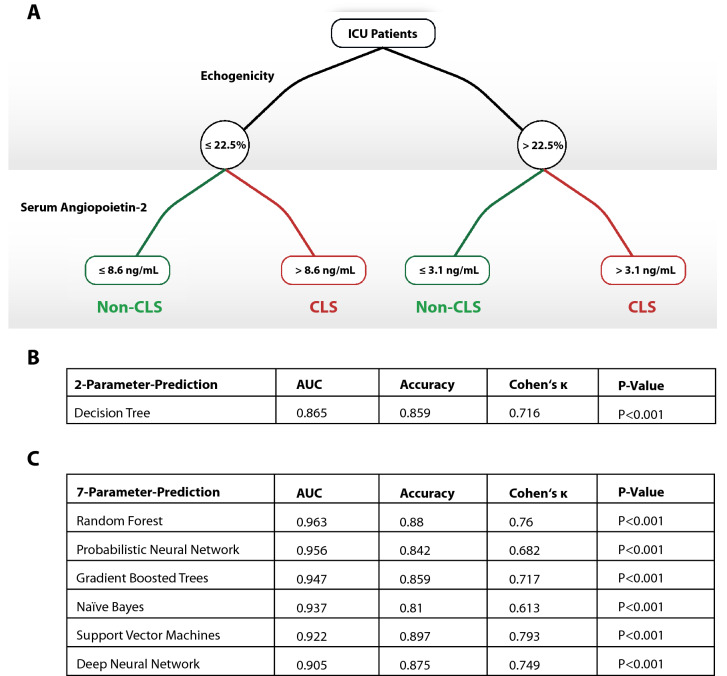
Results: The 30-day mortility was increased among CLS patients (12 vs. 1%, P = 0.002), while showing higher SOFA-scores. Extracellular water was increased in patients with CLS with higher echogenicity of subcutaneous tissue [29(24-31) vs. 19(16-21), P < 0.001]. Biomarkers showed characteristic alterations, especially with an increased angiopoietin-2 concentration in CLS [9.9(6.2-17.3) vs. 3.7(2.6-5.6)ng/mL, P < 0.001]. We developed a score using seven parameters (echogenicity, SOFA-score, angiopoietin-2, syndecan-1, ICAM-1, lactate and interleukin-6). A Random Forest prediction model boosted its diagnostic characteristics (AUC 0.963, P < 0.001), while a two-parameter decision tree model showed good specifications (AUC 0.865).
Conclusions: Diagnosis of CLS in critically ill patients is feasible by objective, non-invasive parameters using the CLS-Score. A simplified two-parameter diagnostic approach can enhance clinical utility. CLS contributes to mortality and should, therefore, classified as an independent entity.
Trial registration: German Clinical Trials Registry (DRKS No. 00012713), Date of registration 10/05/2017, www.drks.de.
Keywords: Capillary leak syndrome; Critical care; Endothelial permeability; Fluid balance; Sepsis.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Marx G, Vangerow B, Burczyk C, Gratz KF, Maassen N, Meyer MC, et al. Evaluation of noninvasive determinants for capillary leakage syndrome in septic shock patients. Intensiv Care Med. 2000;26:1252–1258. - PubMed
-
- Schlegel N, Leweke R, Meir M, Germer C-T, Waschke J. Role of NF-κB activation in LPS-induced endothelial barrier breakdown. Histochem Cell Biol. 2012;138:627–641. - PubMed
-
- Schlegel N, Waschke J. Vasodilator-stimulated phosphoprotein: crucial for activation of Rac1 in endothelial barrier maintenance. Cardiovasc Res. 2010;87:1–3. - PubMed
-
- Lee WL, Slutsky AS. Sepsis and endothelial permeability. N Engl J Med. 2010;363:689–691. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
