

Walking-adaptability therapy after stroke: results of a randomized controlled trial
- PMID: 34911566
- PMCID: PMC8672482
- DOI: 10.1186/s13063-021-05742-3
Walking-adaptability therapy after stroke: results of a randomized controlled trial
Abstract
Background: The ability to adapt walking to environmental properties and hazards, a prerequisite for safe ambulation, is often impaired in persons after stroke.
Research question: The aim of this study was to compare the efficacy of two walking-adaptability interventions: a novel treadmill-based C-Mill therapy (using gait-dependent augmented reality) and the standard overground FALLS program (using physical context). We expected sustained improvements for both treatment groups combined but hypothesized better outcomes for C-Mill therapy than the FALLS program due to its expected greater amount of walking practice.
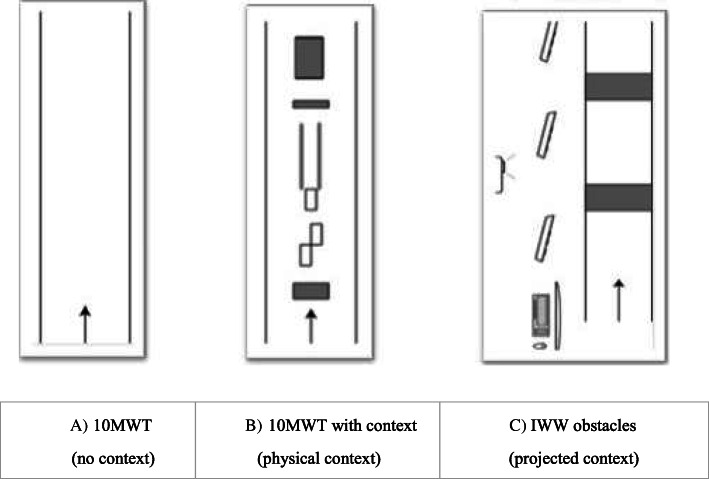
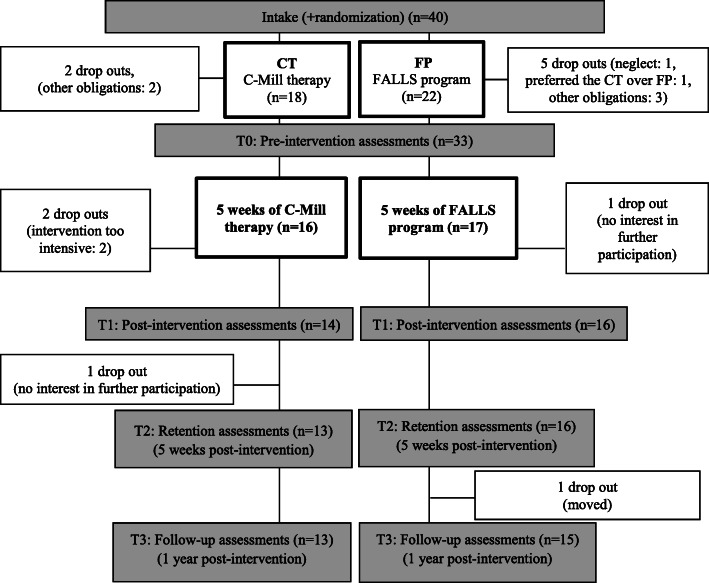
Methods: In this pre-registered single-centre parallel group randomized controlled trial, forty persons after stroke (≥ 3 months ago) with walking and/or balance deficits were randomly allocated to either 5 weeks of C-Mill therapy or the FALLS program. The primary outcome measure was the standard walking speed as determined with the 10-meter walking test (10MWT). Additionally, context-specific walking speed was assessed in environments enriched with either stationary physical context (10MWT context) or suddenly appearing visual images (Interactive Walkway obstacles). The walking-adaptability scores of those enriched walking tests served as secondary outcome measures. Furthermore, a cognitive task was added to all three assessments to evaluate dual-task performance in this context. Finally, the participants' experience and amount of walking practice were scored. The outcome measures were assessed at four test moments: pre-intervention (T0), post-intervention (T1), 5-week post-intervention retention (T2), and 1-year post-intervention follow-up (T3).
Results: No significant group differences were found between the interventions for the primary outcome measure standard walking speed, but we found a greater improvement in context-specific walking speed with stationary physical context of the C-Mill therapy compared to the FALLS program at the post-intervention test, which was no longer significant at retention. Both interventions were well received, but C-Mill therapy scored better on perceived increased fitness than the FALLS program. C-Mill therapy resulted in twice as many steps per session of equal duration than the FALLS program. The "change-over-time" analyses for participants of both interventions combined showed no significant improvements in the standard walking speed; however, significant improvements were found for context-specific walking speed, walking adaptability, and cognitive dual-task performance.
Significance: This study showed no between-group differences between the novel treadmill-based C-Mill therapy and the standard overground FALLS program with respect to the primary outcome measure standard walking speed. However, the greater amount of walking practice observed for the C-Mill group, an essential aspect of effective intervention programs after stroke, may underlie the reported increased perceived fitness and observed increased context-specific walking speed for the C-Mill group directly after the intervention. Although the "change-over-time" results for all participants combined showed no improvement in the standard walking speed, context-specific walking speed and walking adaptability showed sustained improvements after the interventions, underscoring the importance of including walking-adaptability training and assessment in rehabilitation post stroke.
Trial registration: The Netherlands Trial Register NTR4030 . Registered 11 June 2013.
Keywords: Gait; Rehabilitation; Stroke; Therapy; Walking adaptability; Walking speed.
© 2021. The Author(s).
Conflict of interest statement
No conflict of interest. MR and PJB are inventors of rehabilitation treadmills that include visual context for foot placement. Vrije Universiteit Amsterdam granted this invention exclusively to ForceLink (Culemborg, The Netherlands), an industrial partner of Vrije Universiteit Amsterdam. ForceLink merged with Motek (Amsterdam), who is currently the manufacturer of the C-Mill treadmill and assignee of a patent for rehabilitation treadmills with visual context for foot placement, with MR and PJB listed as inventors. MR and PJB did not receive any reimbursements, fees, funding, or salary from ForceLink or Motek, nor did they benefit personally from patent revenues.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
