

Asthma and COVID-19: an update
- PMID: 34911694
- PMCID: PMC8674937
- DOI: 10.1183/16000617.0152-2021
Asthma and COVID-19: an update
Abstract
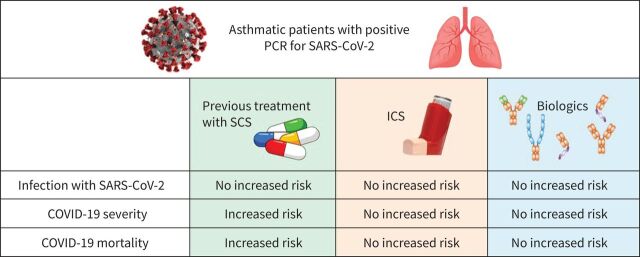
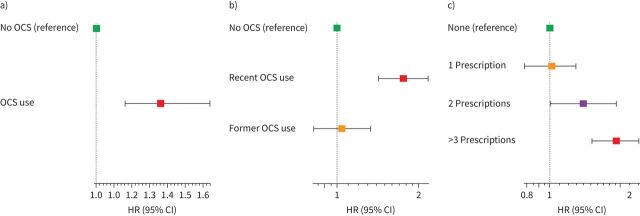
As the world faces the coronavirus disease 2019 (COVID-19) pandemic due to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, concerns have been raised that asthma patients could be at increased risk of SARS-CoV-2 infection and disease severity. However, it appears that asthma is not an independent risk factor for both. Furthermore, asthma is not over-represented in hospitalised patients with severe pneumonia due to SARS-CoV-2 infection and there was no increased risk of asthma exacerbations triggered by SARS-CoV-2. There is accumulating evidence that asthma phenotypes and comorbidities are important factors in evaluating the risk for SARS-CoV-2 infection and disease severity, as findings suggest that Th2-high inflammation may reduce the risk of SARS-Cov-2 infection and disease severity in contrast to increased risk in patients with Th2-low asthma. The use of inhaled corticosteroids (ICS) is safe in asthma patients with SARS-CoV-2 infection. Furthermore, it has been proposed that ICS may confer some degree of protection against SARS-CoV-2 infection and the development of severe disease by reducing the expression of angiotensin converting enzyme-2 and transmembrane protease serine in the lung. In contrast, chronic or recurrent use of systemic corticosteroids before SARS-CoV-2 infection is a major risk factor of poor outcomes and worst survival in asthma patients. Conversely, biological therapy for severe allergic and eosinophilic asthma does not increase the risk of being infected with SARS-CoV-2 or having worse COVID-19 severity. In the present review we will summarise the current literature regarding asthma and COVID-19.
Copyright ©The authors 2021.
Conflict of interest statement
Conflict of interest: Y. Adir reports personal fees from Teva, grants and personal fees from GSK, grants and personal fees from AstraZeneca, personal fees from Sanofi, outside the submitted work. Conflict of interest: W. Saliba has nothing to disclose. Conflict of interest: A. Beurnier reports personal fees from AstraZeneca, personal fees from Sanofi, outside the submitted work. Conflict of interest: M. Humbert reports personal fees from Acceleron, grants and personal fees from Actelion, grants and personal fees from Bayer, personal fees from GSK, personal fees from Merck, personal fees from Novartis, personal fees from AstraZeneca, personal fees from Sanofi, outside the submitted work.
Figures
References
-
- Satia I, Cusack R, Greene JM,et al. Prevalence and contribution of respiratory viruses in the community to rates of emergency department visits and hospitalizations with respiratory tract infections, chronic obstructive pulmonary disease and asthma. PLoS ONE 2020; 15: e0228544. doi: 10.1371/journal.pone.0228544 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous