

Myelofibrosis: Genetic Characteristics and the Emerging Therapeutic Landscape
- PMID: 34911786
- PMCID: PMC9306313
- DOI: 10.1158/0008-5472.CAN-21-2930
Myelofibrosis: Genetic Characteristics and the Emerging Therapeutic Landscape
Abstract
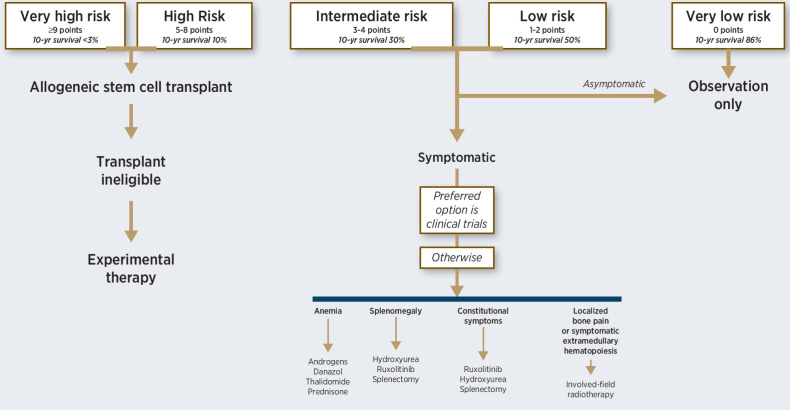
Primary myelofibrosis (PMF) is one of three myeloproliferative neoplasms (MPN) that are morphologically and molecularly inter-related, the other two being polycythemia vera (PV) and essential thrombocythemia (ET). MPNs are characterized by JAK-STAT-activating JAK2, CALR, or MPL mutations that give rise to stem cell-derived clonal myeloproliferation, which is prone to leukemic and, in case of PV and ET, fibrotic transformation. Abnormal megakaryocyte proliferation is accompanied by bone marrow fibrosis and characterizes PMF, while the clinical phenotype is pathogenetically linked to ineffective hematopoiesis and aberrant cytokine expression. Among MPN-associated driver mutations, type 1-like CALR mutation has been associated with favorable prognosis in PMF, while ASXL1, SRSF2, U2AF1-Q157, EZH2, CBL, and K/NRAS mutations have been shown to be prognostically detrimental. Such information has enabled development of exclusively genetic (GIPSS) and clinically integrated (MIPSSv2) prognostic models that facilitate individualized treatment decisions. Allogeneic stem cell transplantation remains the only treatment modality in MF with the potential to prolong survival, whereas drug therapy, including JAK2 inhibitors, is directed mostly at the inflammatory component of the disease and is therefore palliative in nature. Similarly, disease-modifying activity remains elusive for currently available investigational drugs, while their additional value in symptom management awaits controlled confirmation. There is a need for genetic characterization of clinical observations followed by in vitro and in vivo preclinical studies that will hopefully identify therapies that target the malignant clone in MF to improve patient outcomes.
©2021 The Authors; Published by the American Association for Cancer Research.
Figures
References
-
- Dameshek W. Some speculations on the myeloproliferative syndromes. Blood 1951;6:372–5. - PubMed
-
- Swerdlow HS, Campo E, Haris NL, Jaffe ES, Pileri SA, Stein H, et al. . WHO classification of tumours of haematopoietic and lymphoid tissues. Lyon, France: IARC; 2017.
-
- Heuck G. Zwei Falle von Leukamie mit eigenthumlichem Blut- resp. Knochenmarksbefund (Two cases of leukemia with peculiar blood and bone marrow findings, respectively). Arch Pathol Anat Physiol Virchows 1879;78:475–96.
-
- Askanazy M. Ueber extrauterine Bildung von Blutzellen in der Leber. Verh Dtsch Pathol Ges 1904;7:58–65.
-
- Assmann H. Beitrage zur osteosklerotischen anamie. Beitr Pathol Anat Allgemeinen Pathologie 1907;41:565–95.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
