

Ceftriaxone-associated Pseudolithiasis in Elderly People: Frequency and Risk Factors
- PMID: 34911872
- PMCID: PMC8758443
- DOI: 10.2169/internalmedicine.7611-21
Ceftriaxone-associated Pseudolithiasis in Elderly People: Frequency and Risk Factors
Abstract
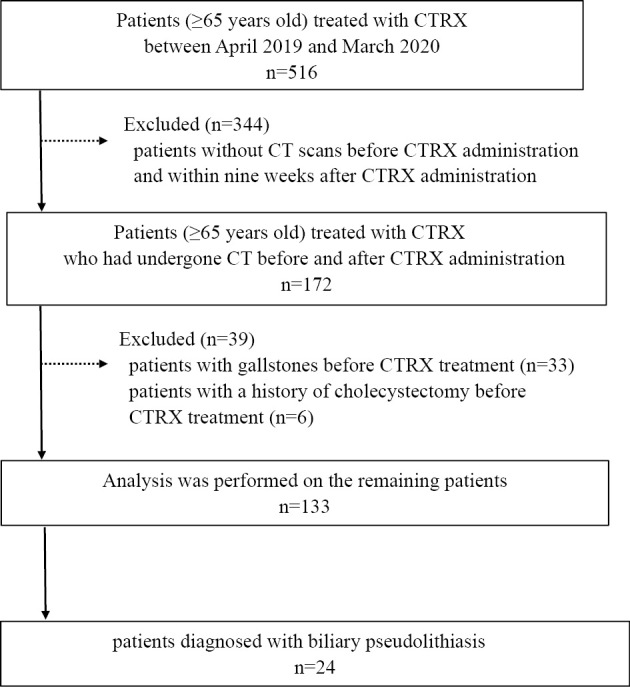
Objective Ceftriaxone (CTRX) is a widely used antibiotic because of its long plasma half-life and good tissue transmission. Many of the reported studies on CTRX-associated pseudolithiasis were performed in children. Although some studies have been published in adults, there are no studies limited to elderly people. The present study investigated CTRX-associated pseudolithiasis and explored its risk factors in the elderly. Methods We retrospectively reviewed 133 elderly patients (≥65 years old) treated with CTRX. Pseudolithiasis was defined as stones or sludge newly appearing in the gallbladder, as detected by computed tomography after the administration of CTRX. We evaluated the risk factors for pseudolithiasis using multivariate regression and inverse probability of treatment weighting analyses. Results Among the 133 patients, 24 (18%) developed CTRX-associated pseudolithiasis. In a multivariate analysis, the CTRX dose [odds ratio (OR) 4.54, 95% confidence interval (CI) 1.36-15.07, p=0.012] and CTRX treatment duration (OR 2.80, 95% CI 1.06-8.04, p=0.043) were significantly associated with pseudolithiasis formation. The cut-off value of the total CTRX dose associated with pseudolithiasis formation was 19 g. A propensity analysis determined that the frequency of pseudolithiasis was increased in patients treated with >19 g total CTRX compared with those who received ≤19 g in total (OR 4.06, 95% CI 1.45-11.32, p=0.008). Conclusion The incidence rate of CTRX-induced pseudolithiasis is high in elderly people, and the CTRX dose and CTRX treatment duration are significant risk factors for pseudolithiasis. A total dose of >19 g increases the likelihood of pseudolithiasis formation in elderly people treated with CTRX.
Keywords: IPTW; ceftriaxone; cut-off value; elderly people; pseudolithiasis.
Conflict of interest statement
Figures

References
-
- Schaad UB, Tschäppeler H, Lentze MJ. Transient formation of precipitations in the gallbladder associated with ceftriaxone therapy. Pediatr Infect Dis 5: 708-710, 1986. - PubMed
-
- Schaad UB, Wedgwood-Krucko J, Tschaeppeler H. Reversible ceftriaxone-associated biliary pseudolithiasis in children. Lancet 332: 1411-1413, 1988. - PubMed
-
- Brogard JM, Blickle JF, Jehl F, Arnaud JP, Paris-Bockel D, Monteil H. High biliary elimination of ceftriaxone in man. Int J Clin Pharmacol Ther Toxicol 26: 167-172, 1988. - PubMed
-
- Riccabona M, Kerbl R, Schwinger W, Spork D, Millner M, Grubbauer HM. Ceftriaxone-induced cholelithiasis--a harmless side-effect? Klin Padiatr 205: 421-423, 1993. - PubMed
-
- Lebovics E, Halata MS, Rosario JA, Lantin J, Schwarz SM, Rosenthal WS. Endoscopic management of ceftriaxone pseudolithiasis involving the common bile duct and gallbladder. Gastrointest Endosc 40: 246-248, 1994. - PubMed