

Molecular pathways in post-colonoscopy versus detected colorectal cancers: results from a nested case-control study
- PMID: 34912077
- PMCID: PMC8927607
- DOI: 10.1038/s41416-021-01619-z
Molecular pathways in post-colonoscopy versus detected colorectal cancers: results from a nested case-control study
Abstract
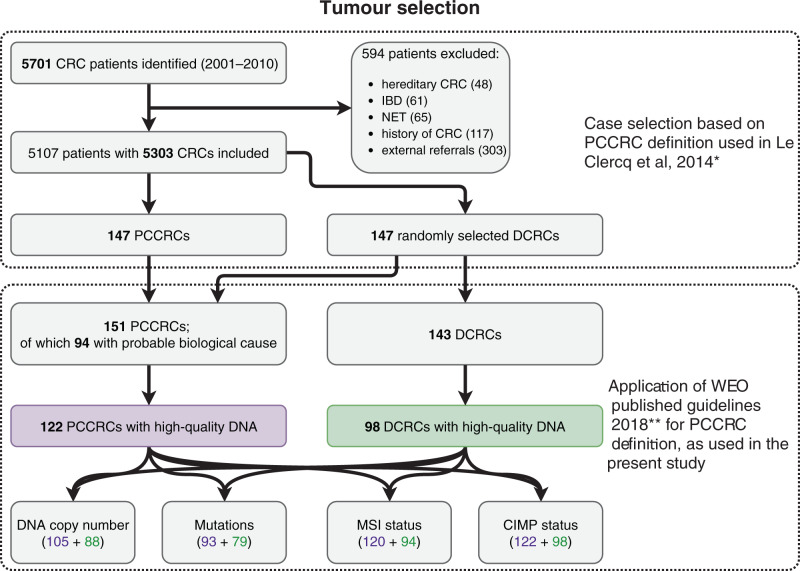
Background: Post-colonoscopy colorectal cancers (PCCRCs) pose challenges in clinical practice. PCCRCs occur due to a combination of procedural and biological causes. In a nested case-control study, we compared clinical and molecular features of PCCRCs and detected CRCs (DCRCs).
Methods: Whole-genome chromosomal copy number changes and mutation status of genes commonly affected in CRC were examined by low-coverage WGS and targeted sequencing, respectively. MSI and CIMP status was also determined.
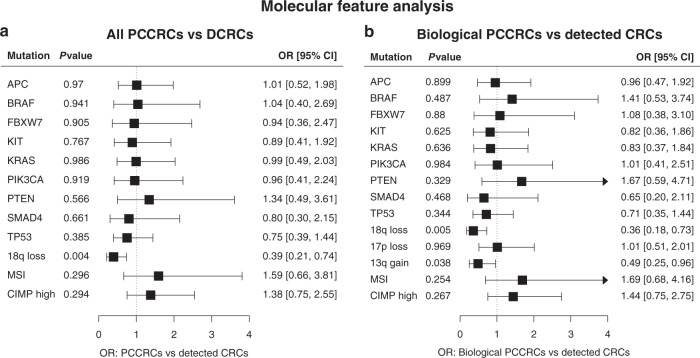
Results: In total, 122 PCCRCs and 98 DCRCs with high-quality DNA were examined. PCCRCs were more often located proximally (P < 0.001), non-polypoid appearing (P = 0.004), early stage (P = 0.009) and poorly differentiated (P = 0.006). PCCRCs showed significantly less 18q loss (FDR < 0.2), compared to DCRCs. No significant differences in mutations were observed. PCCRCs were more commonly CIMP high (P = 0.014) and MSI (P = 0.029). After correction for tumour location, only less 18q loss remained significant (P = 0.005).
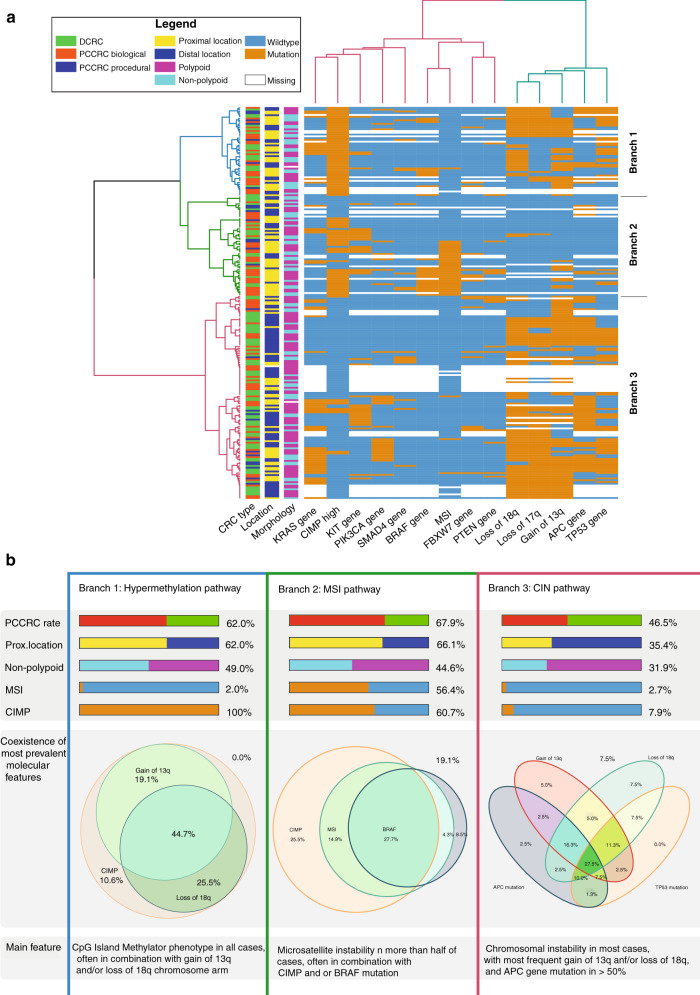
Conclusion: Molecular features associated with the sessile serrated lesions (SSLs) and non-polypoid colorectal neoplasms (CRNs) are more commonly seen in PCCRCs than in DCRCs. These together with the clinical features observed support the hypothesis that SSLs and non-polypoid CRNs are contributors to the development of PCCRCs. The future focus should be directed at improving the detection and endoscopic removal of these non-polypoid CRN and SSLs.
Clinical trial registration: NTR3093 in the Dutch trial register ( www.trialregister.nl ).
© 2021. The Author(s), under exclusive licence to Springer Nature Limited.
Conflict of interest statement
AM received funding from the Dutch Cancer Society, from the Dutch Organization for Health Research and Development, from Pentax Europe GmBH. AM has given scientific advice to Kyowa Kirin, Bayer, and Takeda. BC has several patents pending. The remaining authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
