

The KEYNOTE-811 trial of dual PD-1 and HER2 blockade in HER2-positive gastric cancer
- PMID: 34912120
- PMCID: PMC8959470
- DOI: 10.1038/s41586-021-04161-3
The KEYNOTE-811 trial of dual PD-1 and HER2 blockade in HER2-positive gastric cancer
Abstract
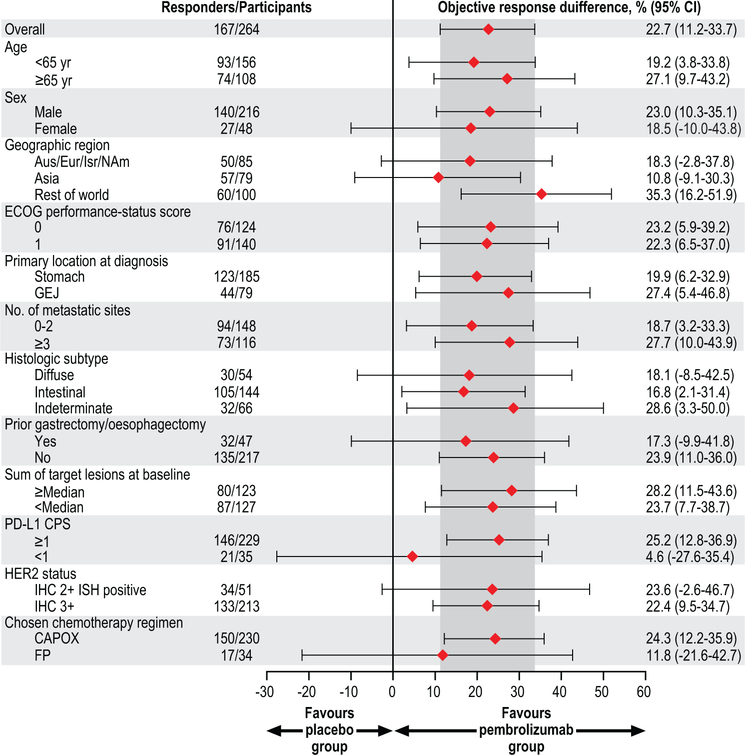
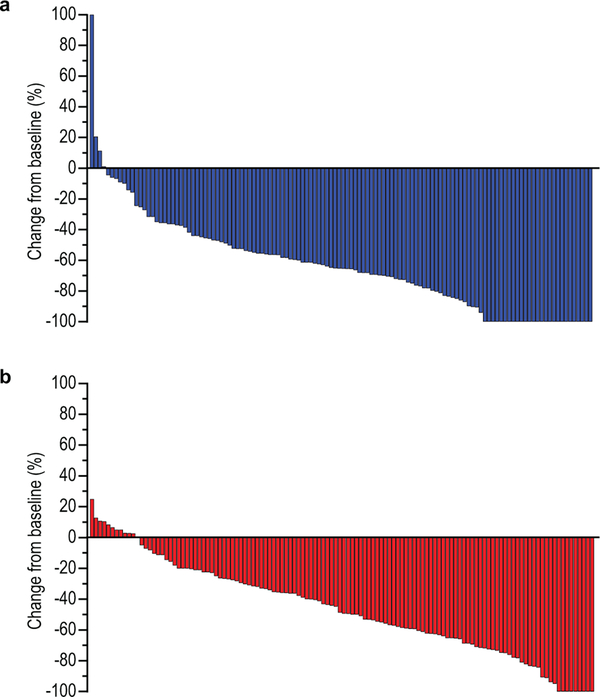
Human epidermal growth factor receptor 2 (HER2, also known as ERBB2) amplification or overexpression occurs in approximately 20% of advanced gastric or gastro-oesophageal junction adenocarcinomas1-3. More than a decade ago, combination therapy with the anti-HER2 antibody trastuzumab and chemotherapy became the standard first-line treatment for patients with these types of tumours4. Although adding the anti-programmed death 1 (PD-1) antibody pembrolizumab to chemotherapy does not significantly improve efficacy in advanced HER2-negative gastric cancer5, there are preclinical6-19 and clinical20,21 rationales for adding pembrolizumab in HER2-positive disease. Here we describe results of the protocol-specified first interim analysis of the randomized, double-blind, placebo-controlled phase III KEYNOTE-811 study of pembrolizumab plus trastuzumab and chemotherapy for unresectable or metastatic, HER2-positive gastric or gastro-oesophageal junction adenocarcinoma22 ( https://clinicaltrials.gov , NCT03615326). We show that adding pembrolizumab to trastuzumab and chemotherapy markedly reduces tumour size, induces complete responses in some participants, and significantly improves objective response rate.
© 2021. The Author(s), under exclusive licence to Springer Nature Limited.
Figures
Comment in
-
Stomach cancer gets a triple punch of therapy.Nature. 2021 Dec;600(7890):608-609. doi: 10.1038/d41586-021-03458-7. Nature. 2021. PMID: 34912062 No abstract available.
-
Pembrolizumab for HER2+ gastric cancer.Nat Rev Clin Oncol. 2022 Mar;19(3):150. doi: 10.1038/s41571-021-00594-x. Nat Rev Clin Oncol. 2022. PMID: 34937950 No abstract available.
-
KEYNOTE-811: pembrolizumab in advanced HER2+ gastric cancer.Nat Rev Gastroenterol Hepatol. 2022 Feb;19(2):79. doi: 10.1038/s41575-022-00577-y. Nat Rev Gastroenterol Hepatol. 2022. PMID: 35017675 No abstract available.
-
Pembrolizumab in HER2-Positive Gastric Cancer.N Engl J Med. 2024 Oct 10;391(14):1360-1362. doi: 10.1056/NEJMc2408121. Epub 2024 Sep 14. N Engl J Med. 2024. PMID: 39282917 Free PMC article. Clinical Trial. No abstract available.
References
Main Text References
-
- Bang YJ et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet 376, 687–697 (2010). - PubMed
Methods References
-
- Eisenhauer EA et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer 45, 228–247 (2009). - PubMed
-
- Oken MM et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol 5, 649–655 (1982). - PubMed
-
- Kulangara K et al. Clinical utility of the combined positive score for programmed death ligand-1 expression and the approval of pembrolizumab for treatment of gastric cancer. Arch Pathol Lab Med 143, 330–337 (2019). - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
