

Combined simultaneous FDG-PET/MRI with T1 and T2 mapping as an imaging biomarker for the diagnosis and prognosis of suspected cardiac sarcoidosis
- PMID: 34913098
- PMCID: PMC8674394
- DOI: 10.1186/s41824-021-00119-w
Combined simultaneous FDG-PET/MRI with T1 and T2 mapping as an imaging biomarker for the diagnosis and prognosis of suspected cardiac sarcoidosis
Abstract
Purpose: To evaluate the diagnostic and prognostic significance of combined cardiac 18F-fluorodeoxyglucose (FDG) PET/MRI with T1/T2 mapping in the evaluation of suspected cardiac sarcoidosis.
Methods: Patients with suspected cardiac sarcoidosis were prospectively enrolled for cardiac 18F-FDG PET/MRI, including late gadolinium enhancement (LGE) and T1/T2 mapping with calculation of extracellular volume (ECV). The final diagnosis of cardiac sarcoidosis was established using modified JMHW guidelines. Major adverse cardiac events (MACE) were assessed as a composite of cardiovascular death, ventricular tachyarrhythmia, bradyarrhythmia, cardiac transplantation or heart failure. Statistical analysis included Cox proportional hazard models.
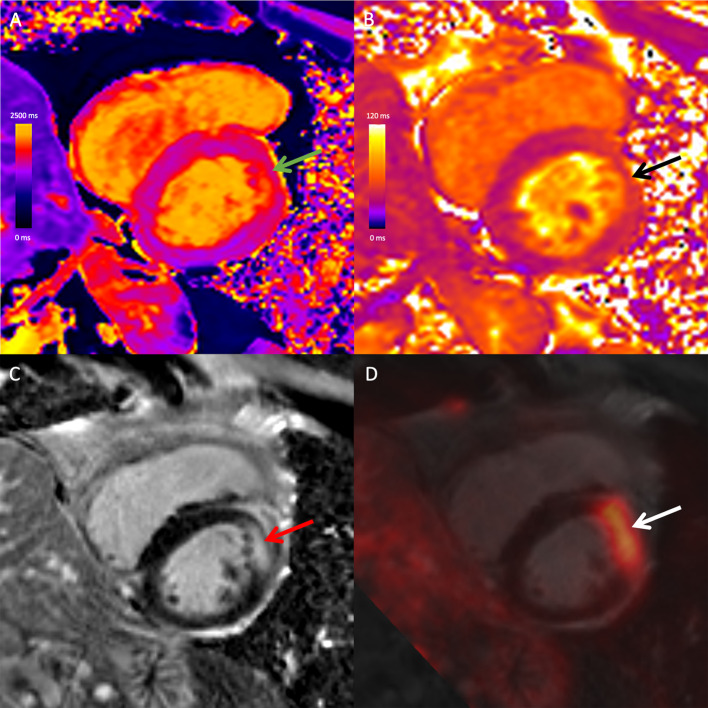
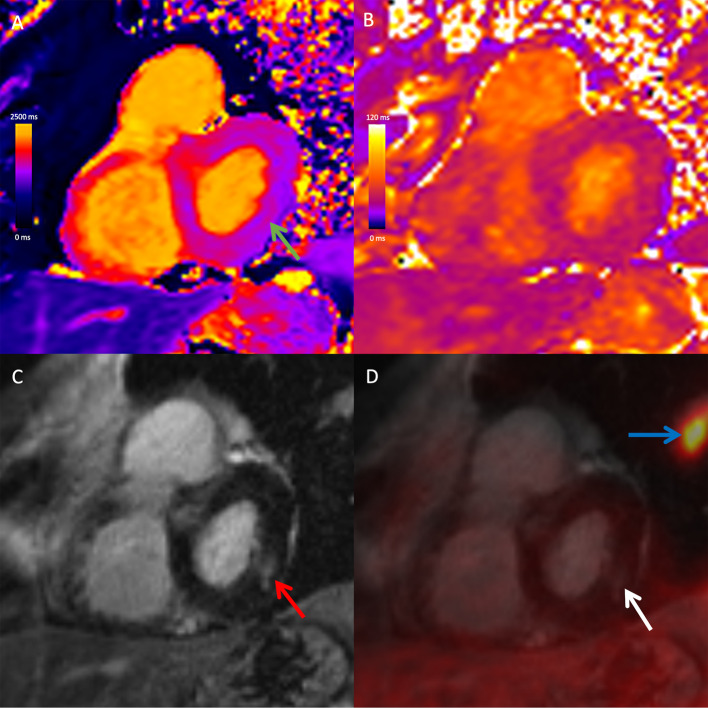
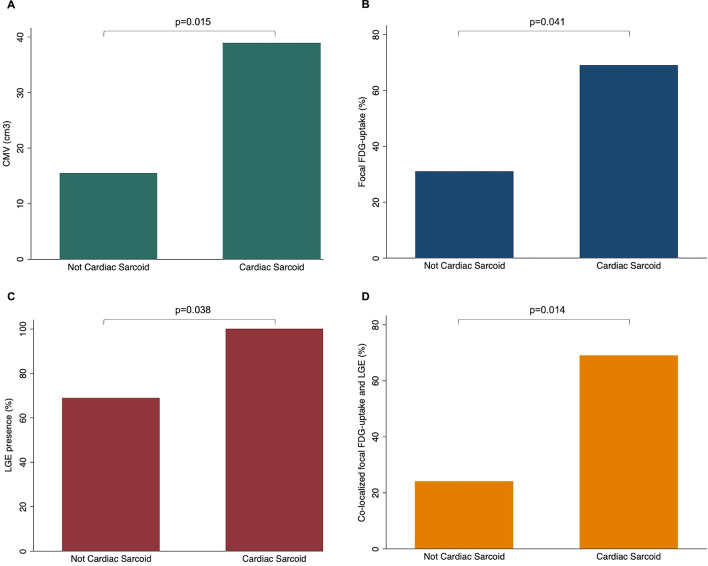
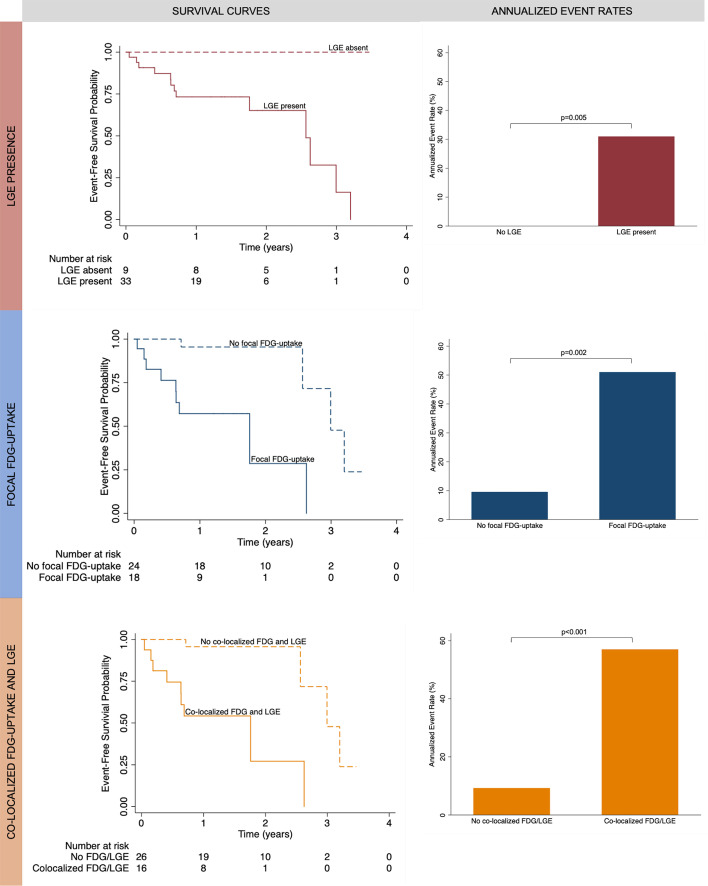
Results: Forty-two patients (53 ± 13 years, 67% male) were evaluated, 13 (31%) with a final diagnosis of cardiac sarcoidosis. Among patients with cardiac sarcoidosis, 100% of patients had at least one abnormality on PET/MRI: FDG uptake in 69%, LGE in 100%, elevated T1 and ECV in 100%, and elevated T2 in 46%. FDG uptake co-localized with LGE in 69% of patients with cardiac sarcoidosis compared to 24% of those without, p = 0.014. Diagnostic specificity for cardiac sarcoidosis was highest for FDG uptake (69%), elevated T2 (79%), and FDG uptake co-localizing with LGE (76%). Diagnostic sensitivity was highest for LGE, elevated T1 and ECV (100%). After median follow-up duration of 634 days, 13 patients experienced MACE. All patients who experienced MACE had LGE, elevated T1 and elevated ECV. FDG uptake (HR 14.7, p = 0.002), elevated T2 (HR 9.0, p = 0.002) and native T1 (HR 1.1 per 10 ms increase, p = 0.044) were significant predictors of MACE even after adjusting for left ventricular ejection fraction and immune suppression treatment. The presence of FDG uptake co-localizing with LGE had the highest diagnostic performance overall (AUC 0.73) and was the best predictor of MACE based on model goodness of fit (HR 14.9, p = 0.001).
Conclusions: Combined cardiac FDG-PET/MRI with T1/T2 mapping provides complementary diagnostic information and predicts MACE in patients with suspected cardiac sarcoidosis.
Keywords: CMR; Cardiac MRI; Cardiac sarcoidosis; FDG PET; PET/MRI; Sarcoidosis.
© 2021. The Author(s).
Conflict of interest statement
Author KH has received a speaker honorarium from Sanofi Genzyme, Amicus and Medscape.
Figures
References
-
- Ahmadian A, Brogan A, Berman J, Sverdlov AL, Mercier G, Mazzini M, et al. Quantitative interpretation of FDG PET/CT with myocardial perfusion imaging increases diagnostic information in the evaluation of cardiac sarcoidosis. J Nucl Cardiol. 2014;21:925–939. doi: 10.1007/s12350-014-9901-9. - DOI - PubMed
-
- Al-Khatib SM, Stevenson WG, Ackerman MJ, Bryant WJ, Callans DJ, Curtis AB, et al. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation. 2018;138:e210–e271. - PubMed
-
- Cerqueira MD, Weissman NJ, Dilsizian V, Jacobs AK, Kaul S, Laskey WK, et al. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Circulation. 2002;105:539–42. doi: 10.1161/hc0402.102975. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Medical