

Unbiased immune profiling reveals a natural killer cell-peripheral nerve axis in fibromyalgia
- PMID: 34913882
- PMCID: PMC8942876
- DOI: 10.1097/j.pain.0000000000002498
Unbiased immune profiling reveals a natural killer cell-peripheral nerve axis in fibromyalgia
Abstract
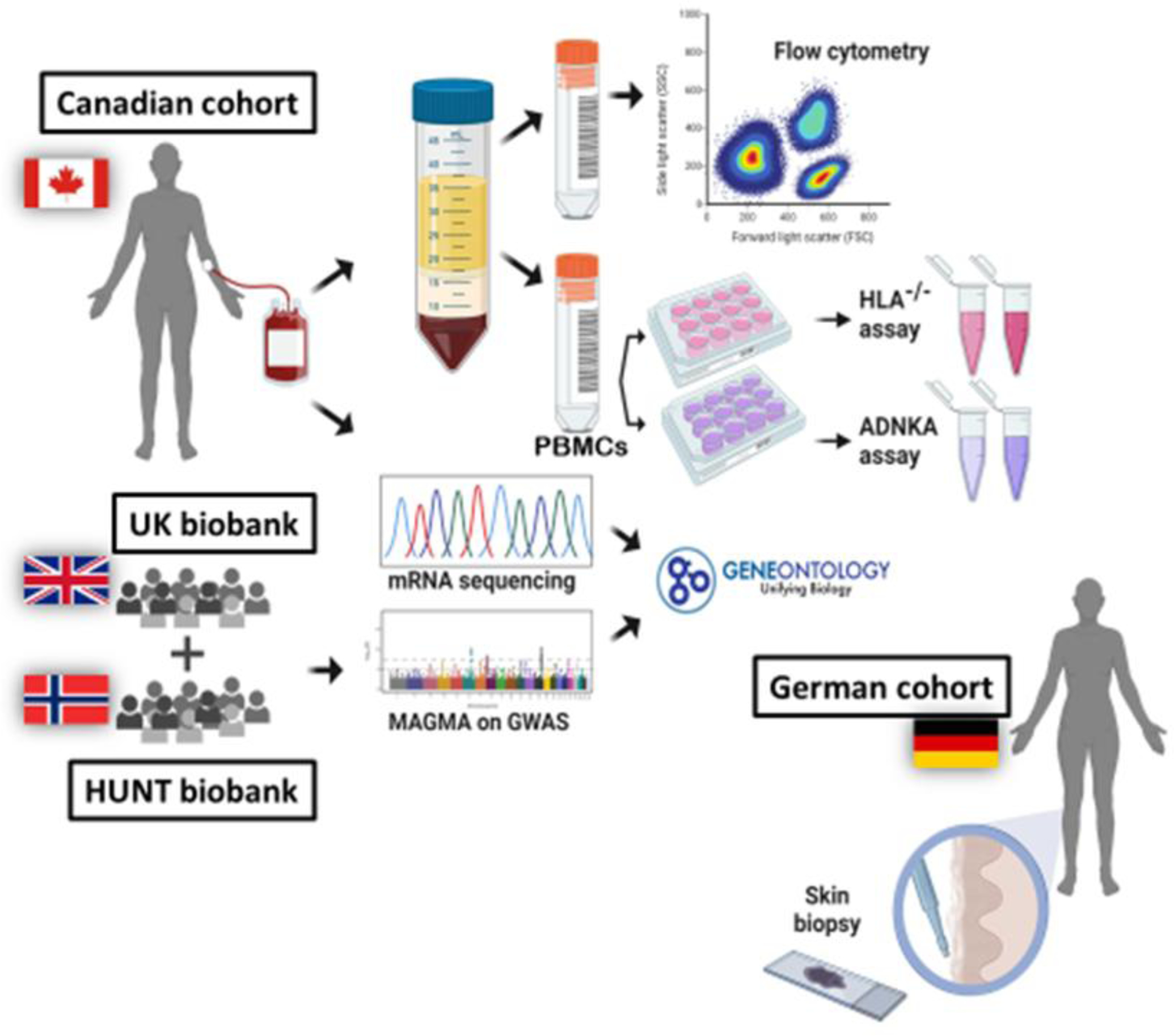
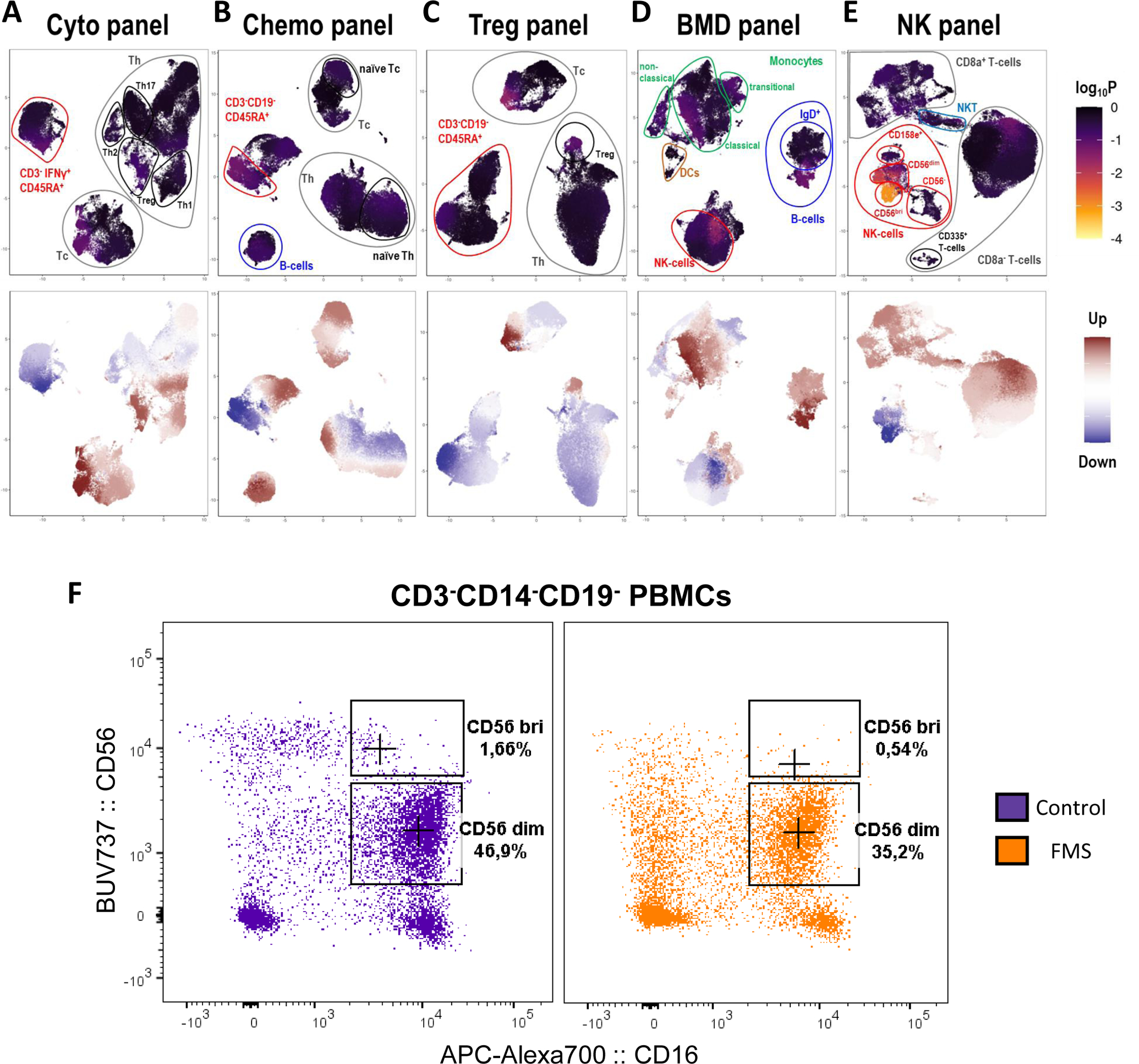
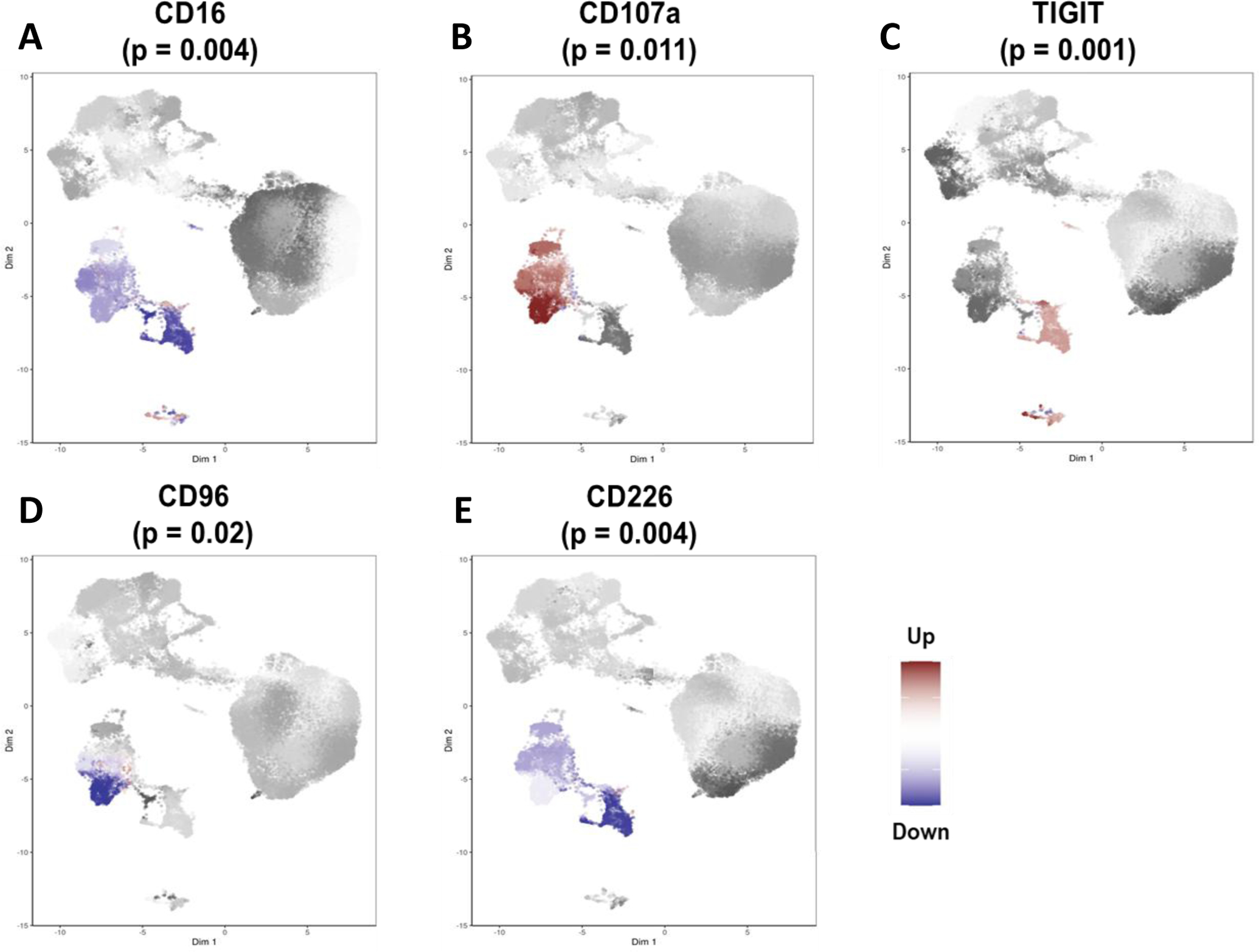
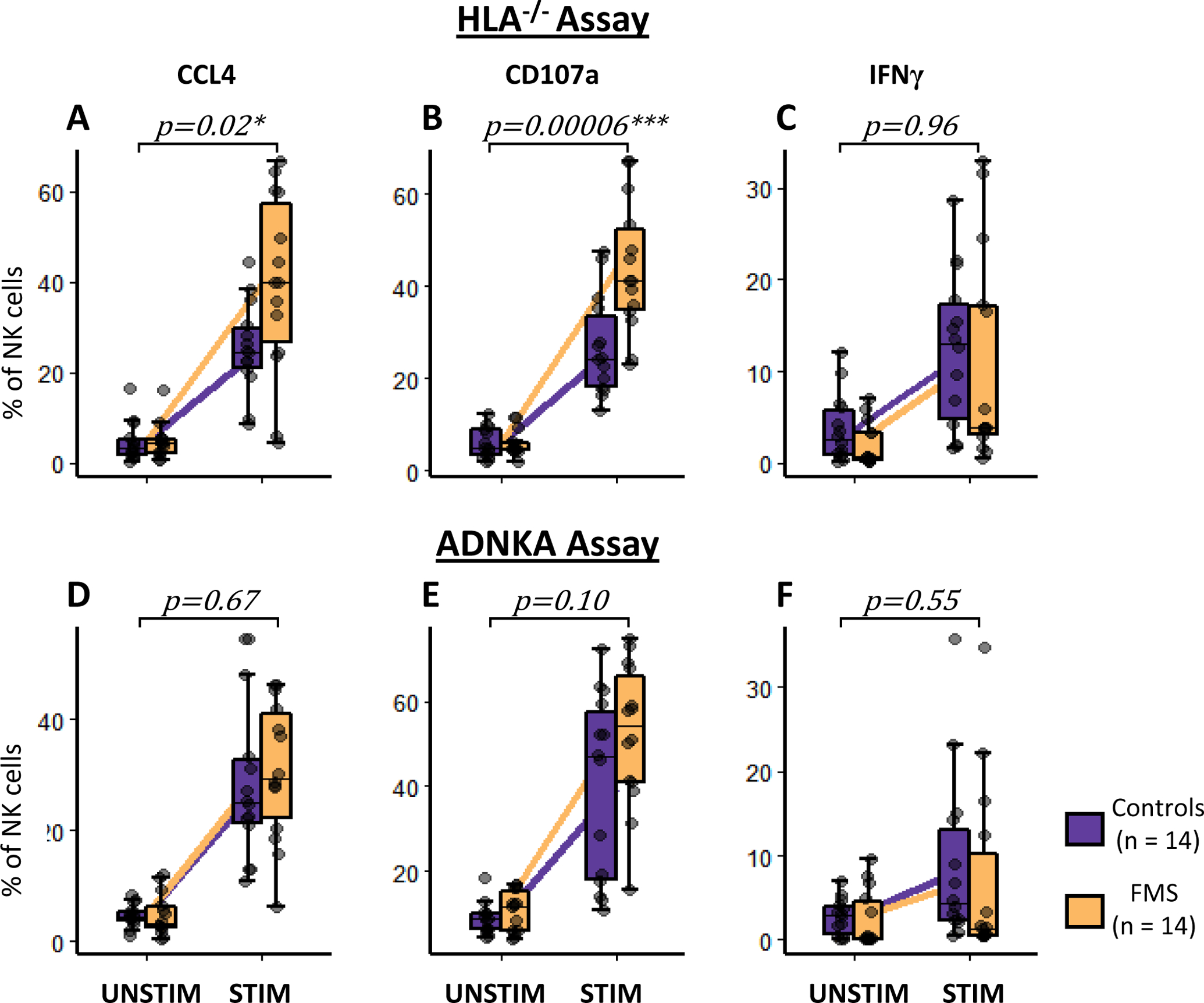
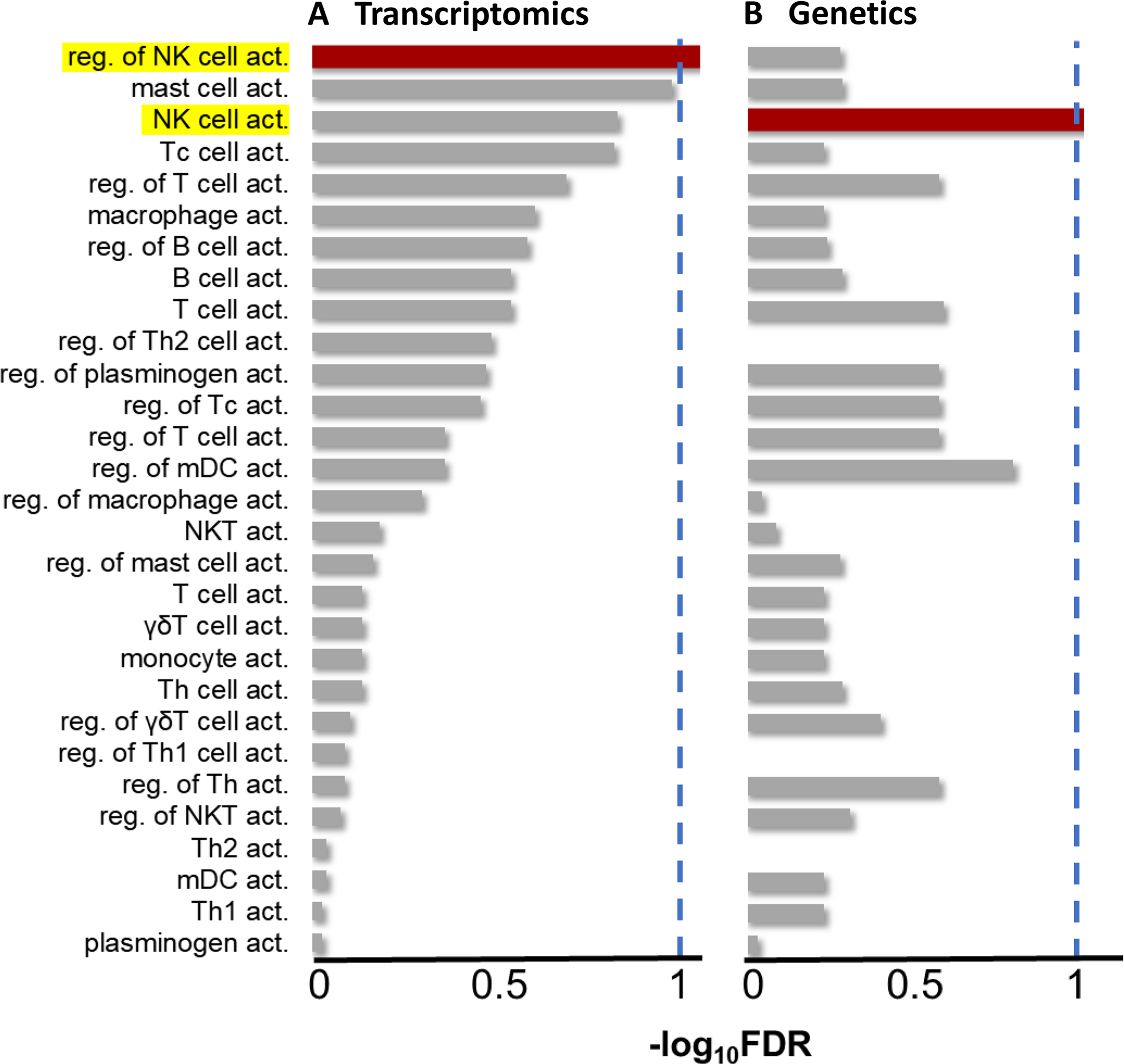
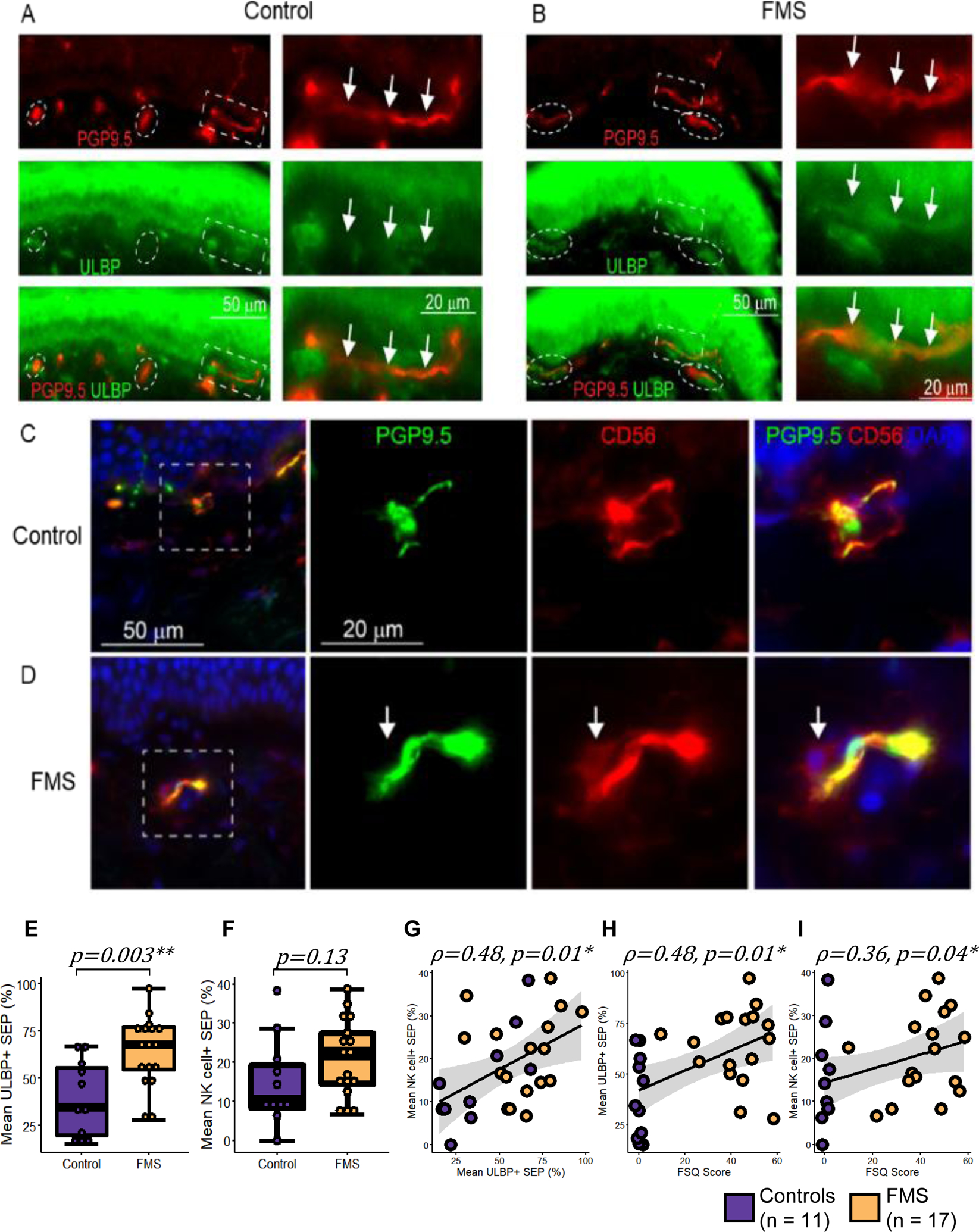
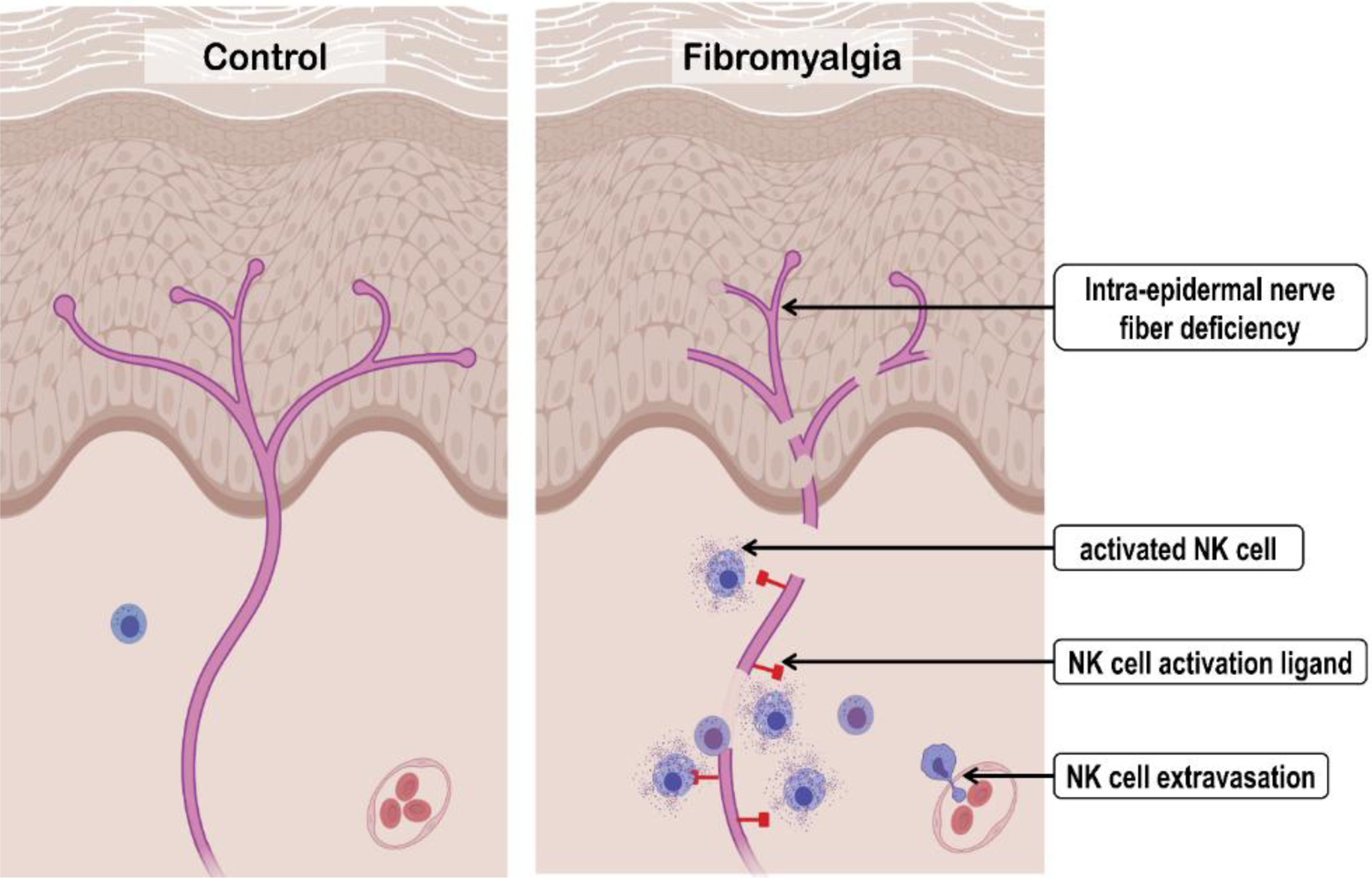
The pathophysiology of fibromyalgia syndrome (FMS) remains elusive, leading to a lack of objective diagnostic criteria and targeted treatment. We globally evaluated immune system changes in FMS by conducting multiparametric flow cytometry analyses of peripheral blood mononuclear cells and identified a natural killer (NK) cell decrease in patients with FMS. Circulating NK cells in FMS were exhausted yet activated, evidenced by lower surface expression of CD16, CD96, and CD226 and more CD107a and TIGIT. These NK cells were hyperresponsive, with increased CCL4 production and expression of CD107a when co-cultured with human leukocyte antigen null target cells. Genetic and transcriptomic pathway analyses identified significant enrichment of cell activation pathways in FMS driven by NK cells. Skin biopsies showed increased expression of NK activation ligand, unique long 16-binding protein, on subepidermal nerves of patients FMS and the presence of NK cells near peripheral nerves. Collectively, our results suggest that chronic activation and redistribution of circulating NK cells to the peripheral nerves contribute to the immunopathology associated with FMS.
Copyright © 2021 International Association for the Study of Pain.
Conflict of interest statement
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- Allen NE, Sudlow C, Peakman T, Collins R, Biobank UK. UK biobank data: come and get it. Sci Transl Med 2014;6(224):224ed224. - PubMed
-
- Andres-Rodriguez L, Borras X, Feliu-Soler A, Perez-Aranda A, Angarita-Osorio N, Moreno-Peral P, Montero-Marin J, Garcia-Campayo J, Carvalho AF, Maes M, Luciano JV. Peripheral immune aberrations in fibromyalgia: A systematic review, meta-analysis and meta-regression. Brain Behav Immun 2020;87:881–889. - PubMed
-
- Arnold LM, Bennett RM, Crofford LJ, Dean LE, Clauw DJ, Goldenberg DL, Fitzcharles MA, Paiva ES, Staud R, Sarzi-Puttini P, Buskila D, Macfarlane GJ. AAPT Diagnostic Criteria for Fibromyalgia. J Pain 2019;20(6):611–628. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
