

Risk of Lymph Node Metastasis in T1b Gastric Cancer: An International Comprehensive Analysis from the Global Gastric Group (G3) Alliance
- PMID: 34913904
- PMCID: PMC9192823
- DOI: 10.1097/SLA.0000000000005332
Risk of Lymph Node Metastasis in T1b Gastric Cancer: An International Comprehensive Analysis from the Global Gastric Group (G3) Alliance
Abstract
Objective: We sought to define criteria associated with low lymph node metastasis risk in patients with submucosal (pT1b) gastric cancer from 3 Western and 3 Eastern countries.
Summary background data: Accurate prediction of lymph node metastasis risk is essential when determining the need for gastrectomy with lymph node dissection following endoscopic resection. Under present guidelines, endoscopic resection is considered definitive treatment if submucosal invasion is only superficial, but this is not routinely assessed.
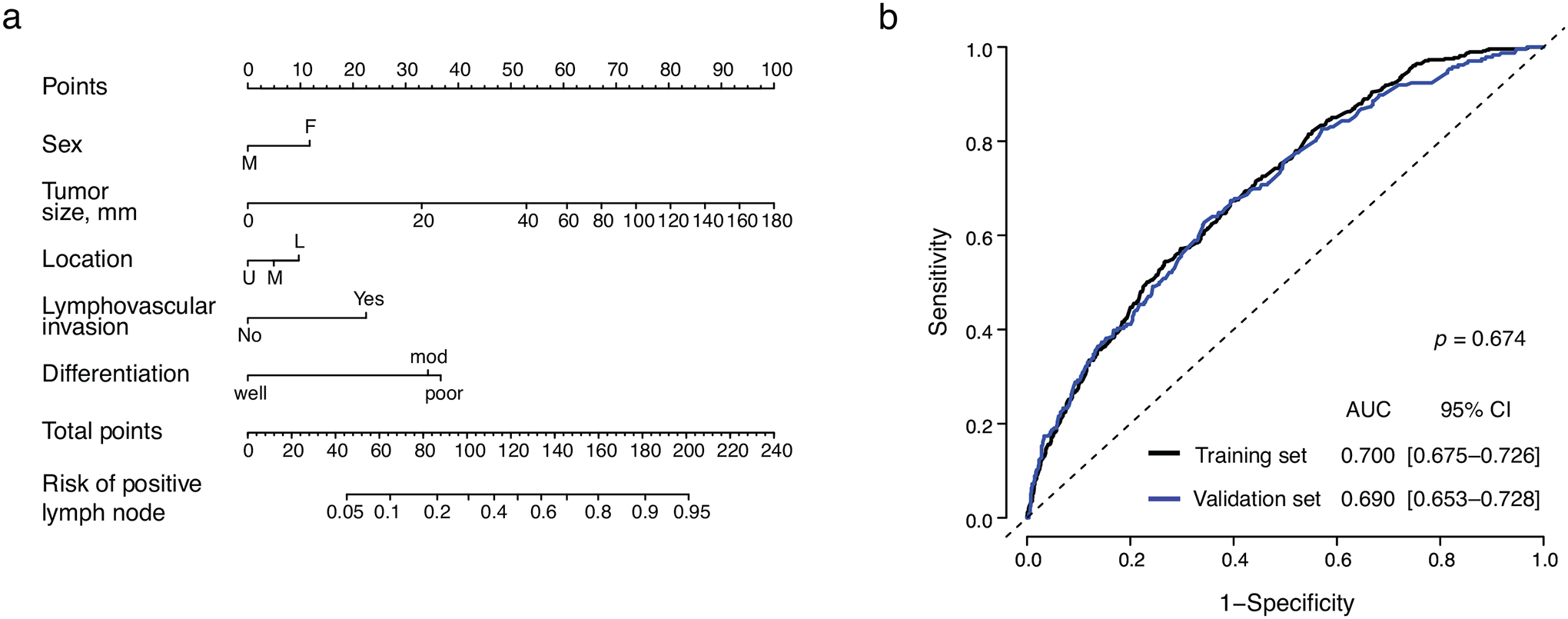
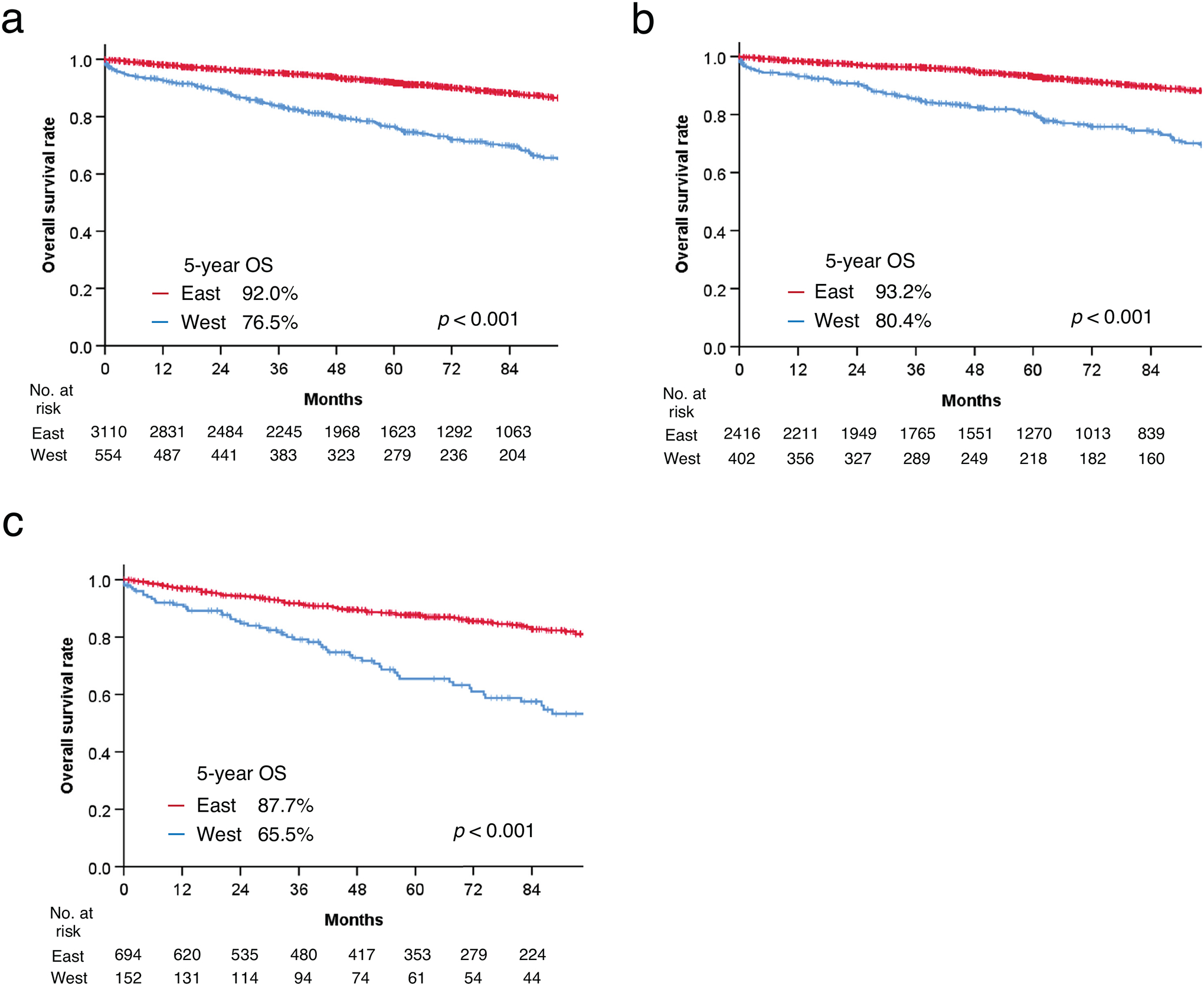
Methods: Lymph node metastasis rates were determined for patient groups defined according to tumor pathological characteristics. Clinicopathological predictors of lymph node metastasis were determined by multivariable logistic regression and used to develop a nomogram in a randomly selected subset that was validated in the remainder. Overall survival was compared between Eastern and Western countries.
Results: Lymph node metastasis was found in 701 of 3166 (22.1%) Eastern and 153 of 560 (27.3%) Western patients. Independent predictors of lymph node metastasis were female sex, tumor size, distal stomach location, lymphovascular invasion, and moderate or poor differentiation. Patients fulfilling the National Comprehensive Cancer Network guideline criteria, excluding the requirement that invasion not extend beyond the superficial submucosa, had a lymph node metastasis rate of 8.9% (53/594). Excluding moderately differentiated tumors lowered the rate to 3.4% (10/296). The nomogram's area under the curve was 0.690. Regardless of lymph node status, overall survival was better in Eastern patients.
Conclusions: The lymph node metastasis rate was lowest in patients with well differentiated tumors that were ≤3 cm and lacked lymphovascular invasion. These criteria may be useful in decisions regarding endoscopic resection as definitive treatment for pT1b gastric cancer.
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Gotoda T Endoscopic resection of early gastric cancer. Gastric Cancer 2007; 10(1):1–11. - PubMed
-
- Ono H, Yao K, Fujishiro M, et al. Guidelines for endoscopic submucosal dissection and endoscopic mucosal resection for early gastric cancer (second edition). Dig Endosc 2020. - PubMed
-
- Gotoda T, Yanagisawa A, Sasako M, et al. Incidence of lymph node metastasis from early gastric cancer: estimation with a large number of cases at two large centers. Gastric Cancer 2000; 3(4):219–225. - PubMed
-
- Ajani JA, D’Amico TA, Almhanna K, et al. Gastric Cancer, Version 3.2016, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw 2016; 14(10):1286–1312. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
