

Estimation of the Timing and Intensity of Reemergence of Respiratory Syncytial Virus Following the COVID-19 Pandemic in the US
- PMID: 34913973
- PMCID: PMC8678706
- DOI: 10.1001/jamanetworkopen.2021.41779
Estimation of the Timing and Intensity of Reemergence of Respiratory Syncytial Virus Following the COVID-19 Pandemic in the US
Abstract
Importance: Respiratory syncytial virus (RSV) is a leading cause of hospitalizations in young children. RSV largely disappeared in 2020 owing to precautions taken because of the COVID-19 pandemic. Estimating the timing and intensity of the reemergence of RSV and the age groups affected is crucial for planning for the administration of prophylactic antibodies and anticipating hospital capacity.
Objective: To examine the association of different factors, including mitigation strategies, duration of maternal-derived immunity, and importation of external infections, with the dynamics of reemergent RSV epidemics.
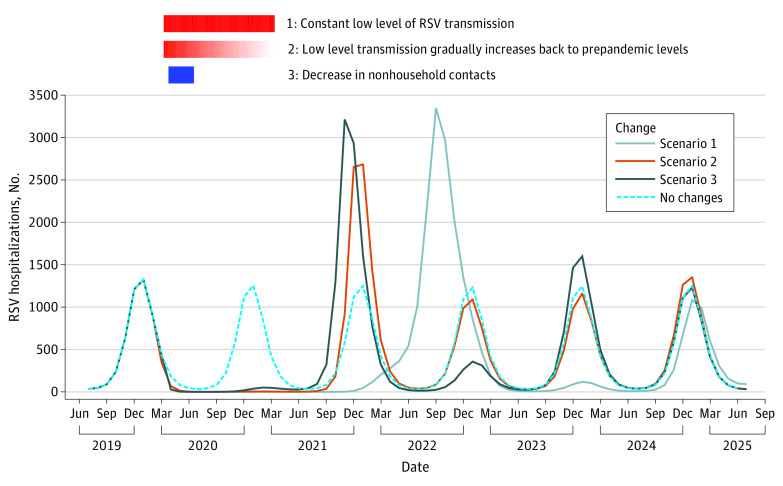
Design, setting, and participants: This simulation modeling study used mathematical models to reproduce the annual epidemics of RSV before the COVID-19 pandemic in New York and California. These models were modified to project the trajectory of RSV epidemics from 2020 to 2025 under different scenarios with varying stringency of mitigation measures for SARS-CoV-2. Simulations also evaluated factors likely to affect the reemergence of RSV epidemics, including introduction of the virus from out-of-state sources and decreased transplacentally acquired immunity in infants. Models using parameters fitted to similar inpatient data sets from Colorado and Florida were used to illustrate these associations in populations with biennial RSV epidemics and year-round RSV circulation, respectively. Statistical analysis was performed from February to October 2021.
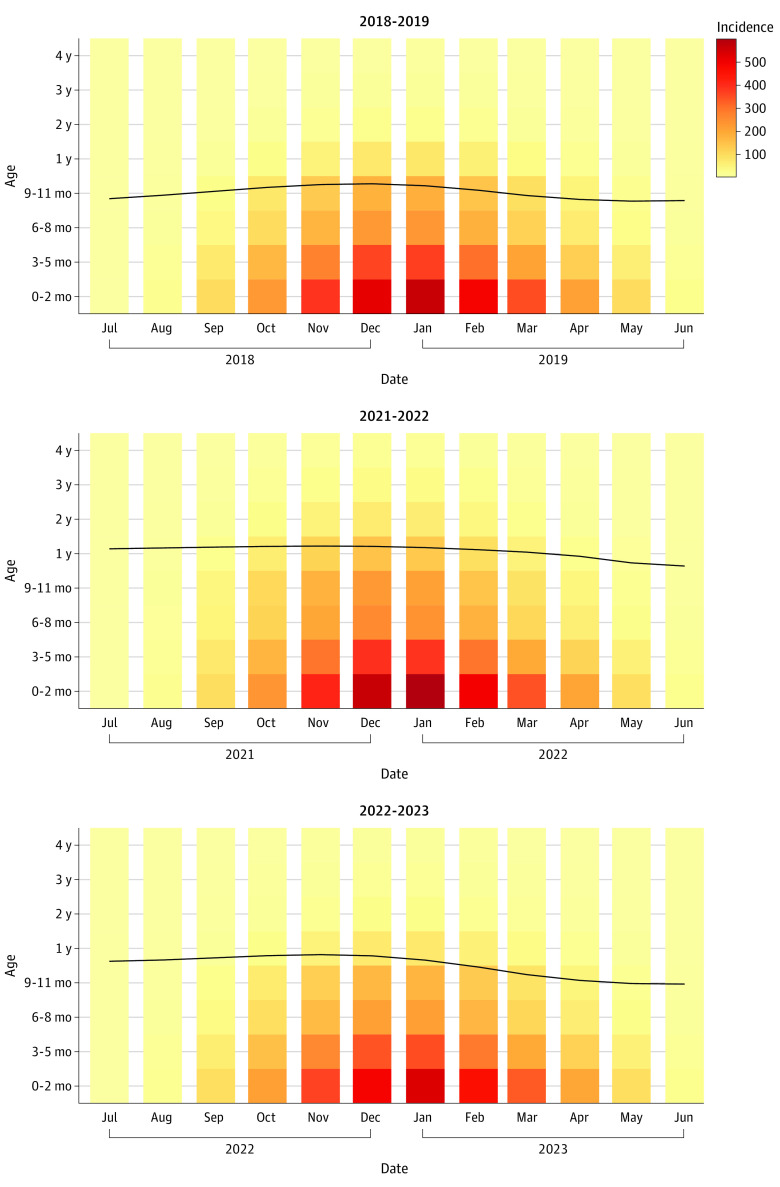
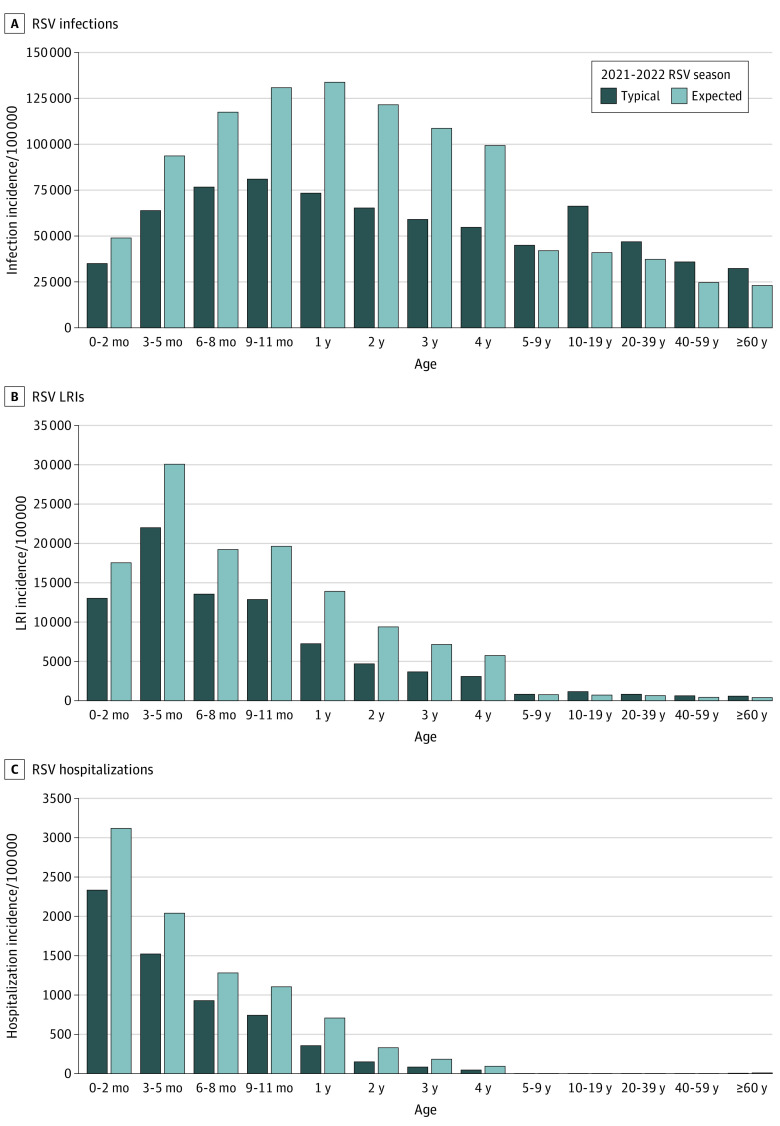
Main outcomes and measures: The primary outcome of this study was defined as the estimated number of RSV hospitalizations each month in the entire population. Secondary outcomes included the age distribution of hospitalizations among children less than 5 years of age, incidence of any RSV infection, and incidence of RSV lower respiratory tract infection.
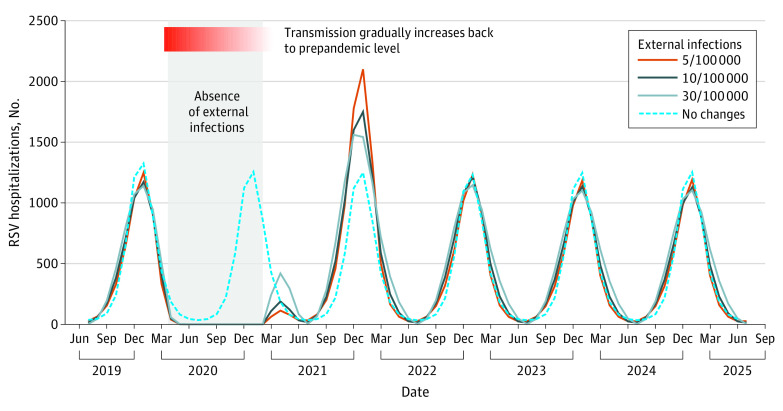
Results: Among a simulated population of 19.45 million people, virus introduction from external sources was associated with the emergence of the spring and summer epidemic in 2021. There was a tradeoff between the intensity of the spring and summer epidemic in 2021 and the intensity of the epidemic in the subsequent winter. Among children 1 year of age, the estimated incidence of RSV hospitalizations was 707 per 100 000 children per year in the 2021 and 2022 RSV season, compared with 355 per 100 000 children per year in a typical RSV season.
Conclusions and relevance: This simulation modeling study found that virus introduction from external sources was associated with the spring and summer epidemics in 2021. These findings suggest that pediatric departments should be alert to large RSV outbreaks in the coming seasons, the intensity of which could depend on the size of the spring and summer epidemic in that location. Enhanced surveillance is recommended for both prophylaxis administration and hospital capacity management.
Conflict of interest statement
Figures
References
-
- Shi T, McAllister DA, O’Brien KL, et al. ; RSV Global Epidemiology Network . Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: a systematic review and modelling study. Lancet. 2017;390(10098):946-958. doi:10.1016/S0140-6736(17)30938-8 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
