

Characterising the dynamics of cerebral metabolic dysfunction following traumatic brain injury: A microdialysis study in 619 patients
- PMID: 34914701
- PMCID: PMC8675704
- DOI: 10.1371/journal.pone.0260291
Characterising the dynamics of cerebral metabolic dysfunction following traumatic brain injury: A microdialysis study in 619 patients
Abstract
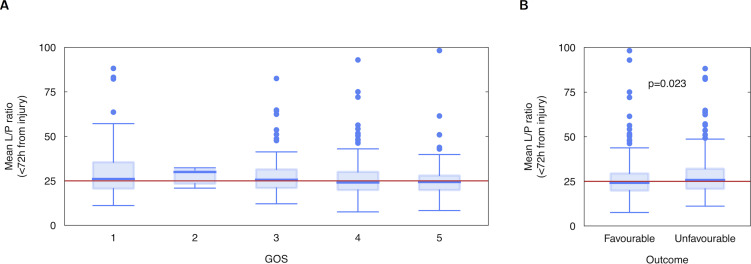
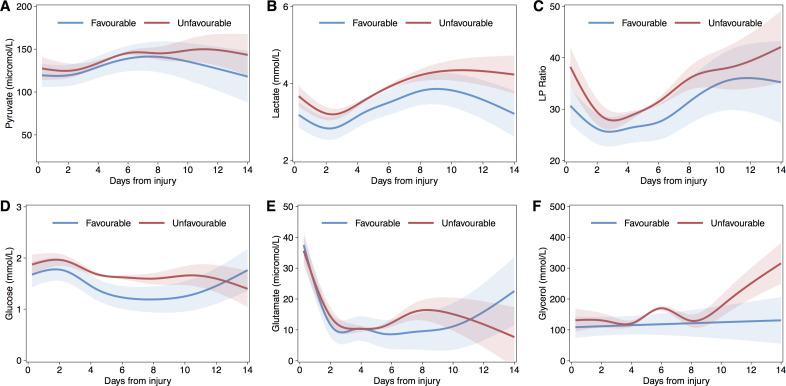
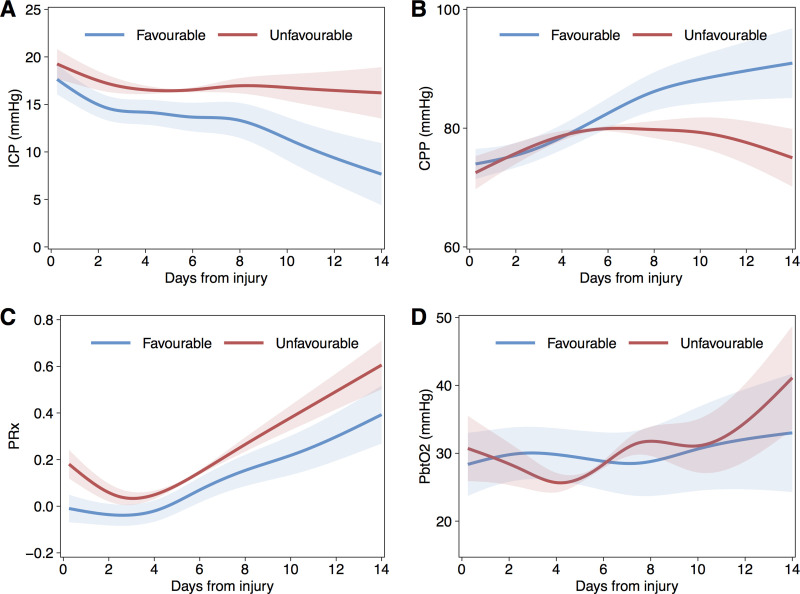
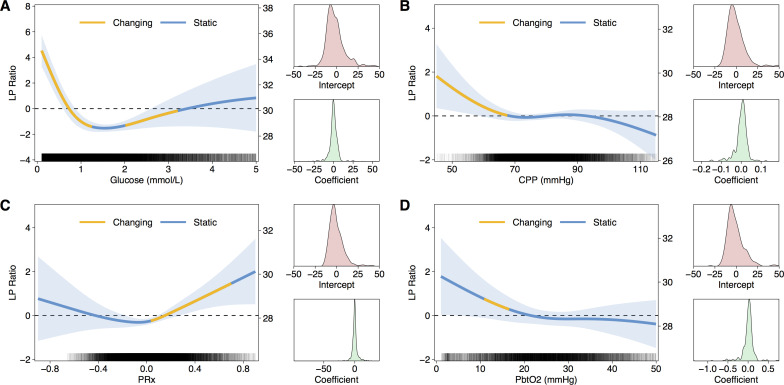
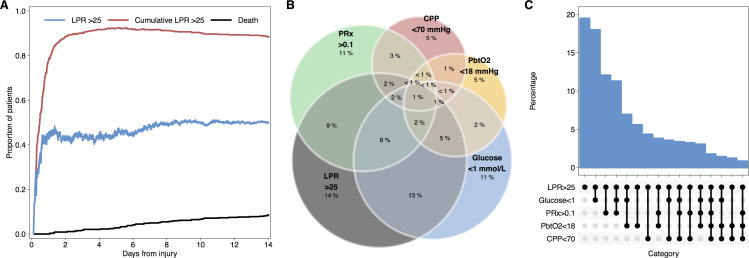
Traumatic brain injury (TBI) is a major cause of death and disability, particularly amongst young people. Current intensive care management of TBI patients is targeted at maintaining normal brain physiology and preventing secondary injury. Microdialysis is an invasive monitor that permits real-time assessment of derangements in cerebral metabolism and responses to treatment. We examined the prognostic value of microdialysis parameters, and the inter-relationships with other neuromonitoring modalities to identify interventions that improve metabolism. This was an analysis of prospective data in 619 adult TBI patients requiring intensive care treatment and invasive neuromonitoring at a tertiary UK neurosciences unit. Patients had continuous measurement of intracranial pressure (ICP), arterial blood pressure (ABP), brain tissue oxygenation (PbtO2), and cerebral metabolism and were managed according to a standardized therapeutic protocol. Microdialysate was assayed hourly for metabolites including glucose, pyruvate, and lactate. Cerebral perfusion pressure (CPP) and cerebral autoregulation (PRx) were derived from the ICP and ABP. Outcome was assessed with the Glasgow Outcome Score (GOS) at 6 months. Relationships between monitoring variables was examined with generalized additive mixed models (GAMM). Lactate/Pyruvate Ratio (LPR) over the first 3 to 7 days following injury was elevated amongst patients with poor outcome and was an independent predictor of ordinal GOS (p<0.05). Significant non-linear associations were observed between LPR and cerebral glucose, CPP, and PRx (p<0.001 to p<0.05). GAMM models suggested improved cerebral metabolism (i.e. reduced LPR with CPP >70mmHg, PRx <0.1, PbtO2 >18mmHg, and brain glucose >1mM. Deranged cerebral metabolism is an important determinant of patient outcome following TBI. Variations in cerebral perfusion, oxygenation and glucose supply are associated with changes in cerebral LPR and suggest therapeutic interventions to improve cerebral metabolism. Future prospective studies are required to determine the efficacy of these strategies.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: PJAH is a director of Technicam (Newton Abbot, UK), the manufacturer of the cranial access device used in this study. MC and PS have financial interest in a part of licensing fee for ICM+ software (Cambridge Enterprise Ltd., UK). This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
