

Blinatumomab maintenance after allogeneic hematopoietic cell transplantation for B-lineage acute lymphoblastic leukemia
- PMID: 34914826
- PMCID: PMC8952188
- DOI: 10.1182/blood.2021013290
Blinatumomab maintenance after allogeneic hematopoietic cell transplantation for B-lineage acute lymphoblastic leukemia
Abstract
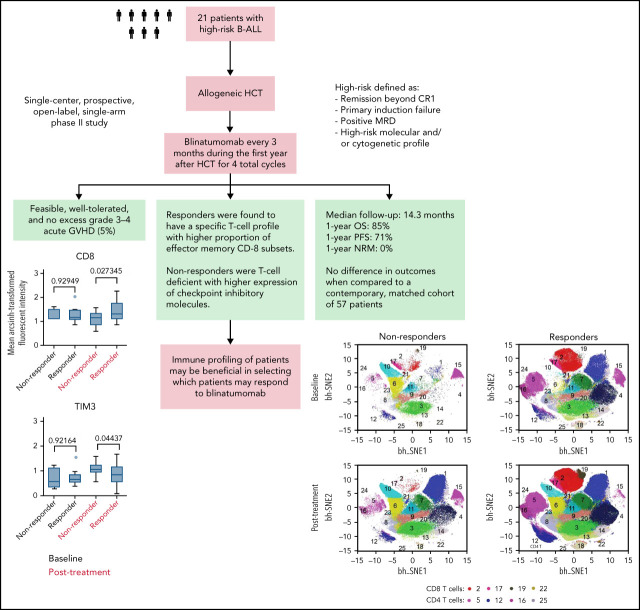
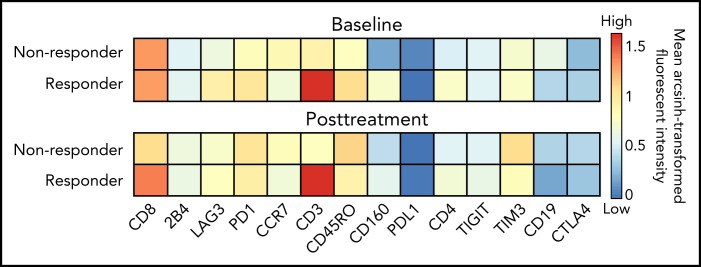
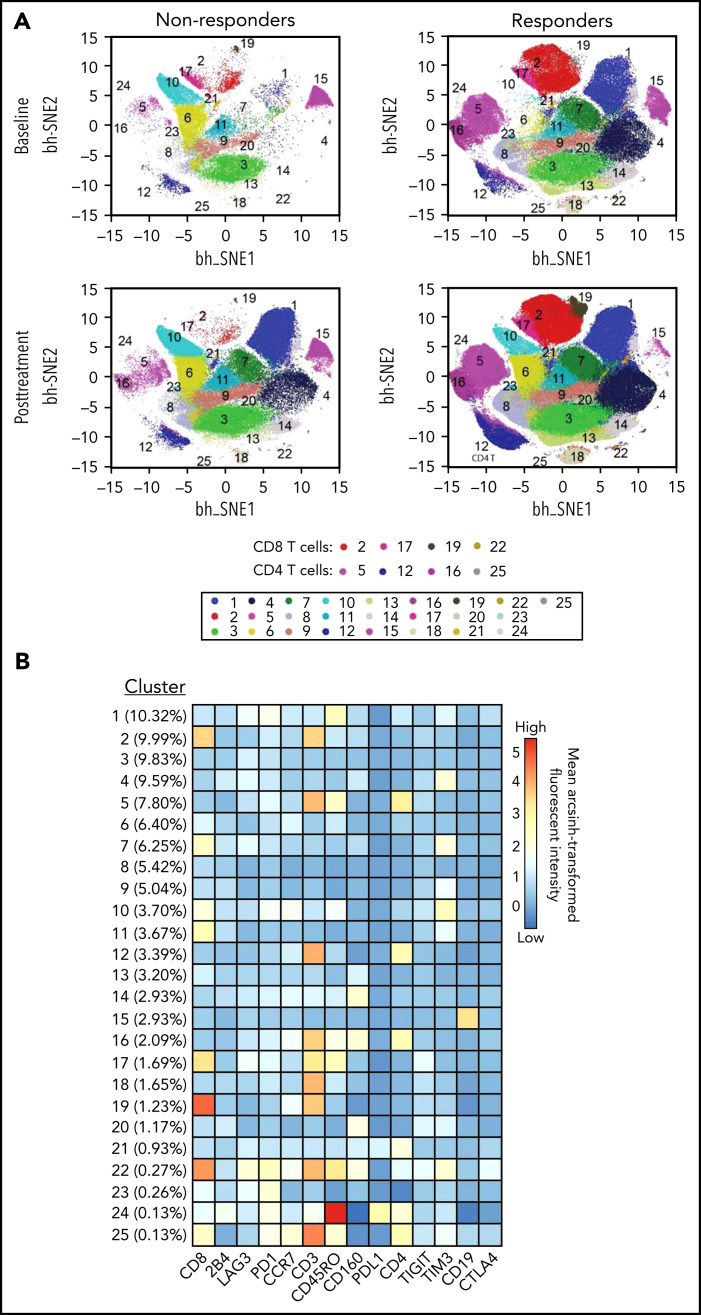
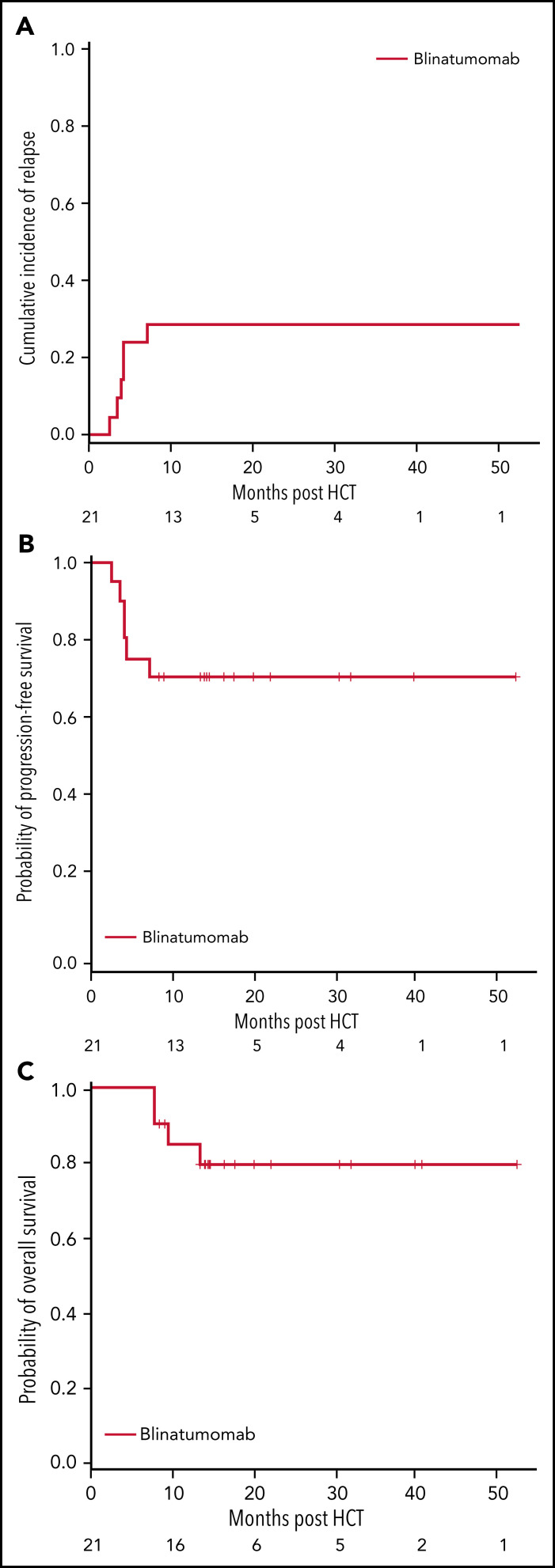
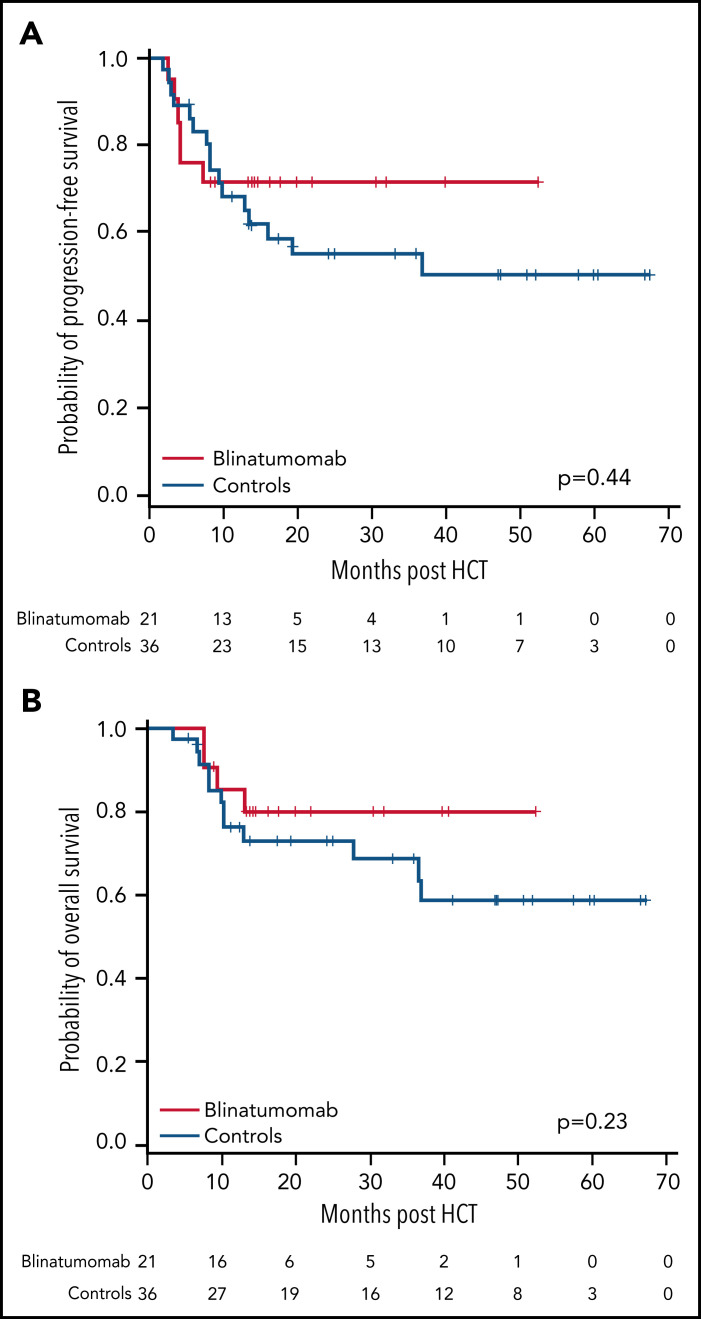
Patients with B-lineage acute lymphoblastic leukemia (ALL) are at high-risk for relapse after allogeneic hematopoietic cell transplantation (HCT). We conducted a single-center phase 2 study evaluating the feasibility of 4 cycles of blinatumomab administered every 3 months during the first year after HCT in an effort to mitigate relapse in high-risk ALL patients. Twenty-one of 23 enrolled patients received at least 1 cycle of blinatumomab and were included in the analysis. The median time from HCT to the first cycle of blinatumomab was 78 days (range, 44 to 105). Twelve patients (57%) completed all 4 treatment cycles. Neutropenia was the only grade 4 adverse event (19%). Rates of cytokine release (5% G1) and neurotoxicity (5% G2) were minimal. The cumulative incidence of acute graft-versus-host disease (GVHD) grades 2 to 4 and 3 to 4 were 33% and 5%, respectively; 2 cases of mild (10%) and 1 case of moderate (5%) chronic GVHD were noted. With a median follow-up of 14.3 months, the 1-year overall survival (OS), progression-free survival (PFS), and nonrelapse mortality (NRM) rates were 85%, 71%, and 0%, respectively. In a matched analysis with a contemporary cohort of 57 patients, we found no significant difference between groups regarding blinatumomab's efficacy. Correlative studies of baseline and posttreatment samples identified patients with specific T-cell profiles as "responders" or "nonresponders" to therapy. Responders had higher proportions of effector memory CD8 T-cell subsets. Nonresponders were T-cell deficient and expressed more inhibitory checkpoint molecules, including T-cell immunoglobulin and mucin domain 3 (TIM3). We found that blinatumomab postallogeneic HCT is feasible, and its benefit is dependent on the immune milieu at time of treatment. This paper is posted on ClinicalTrials.gov, study ID: NCT02807883.
© 2022 by The American Society of Hematology.
Figures
References
-
- Goldstone AH, Richards SM, Lazarus HM, et al. In adults with standard-risk acute lymphoblastic leukemia, the greatest benefit is achieved from a matched sibling allogeneic transplantation in first complete remission, and an autologous transplantation is less effective than conventional consolidation/maintenance chemotherapy in all patients: final results of the International ALL Trial (MRC UKALL XII/ECOG E2993). Blood. 2008;111(4):1827-1833. - PubMed
-
- Fielding AK, Rowe JM, Richards SM, et al. Prospective outcome data on 267 unselected adult patients with Philadelphia chromosome-positive acute lymphoblastic leukemia confirms superiority of allogeneic transplantation over chemotherapy in the pre-imatinib era: results from the International ALL Trial MRC UKALLXII/ECOG2993. Blood. 2009;113(19):4489-4496. - PMC - PubMed
-
- Gökbuget N, Kneba M, Raff T, et al. ; German Multicenter Study Group for Adult Acute Lymphoblastic Leukemia . Adult patients with acute lymphoblastic leukemia and molecular failure display a poor prognosis and are candidates for stem cell transplantation and targeted therapies. Blood. 2012;120(9): 1868-1876. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
