

Apolipoprotein A-IV concentrations and clinical outcomes in a large chronic kidney disease cohort: Results from the GCKD study
- PMID: 34914850
- PMCID: PMC9305919
- DOI: 10.1111/joim.13437
Apolipoprotein A-IV concentrations and clinical outcomes in a large chronic kidney disease cohort: Results from the GCKD study
Abstract
Background: Chronic kidney disease (CKD) represents a chronic proinflammatory state and is associated with very high cardiovascular risk. Apolipoprotein A-IV (apoA-IV) has antiatherogenic, antioxidative, anti-inflammatory and antithrombotic properties and levels increase significantly during the course of CKD.
Objectives: We aimed to investigate the association between apoA-IV and all-cause mortality and cardiovascular outcomes in the German Chronic Kidney Disease study.
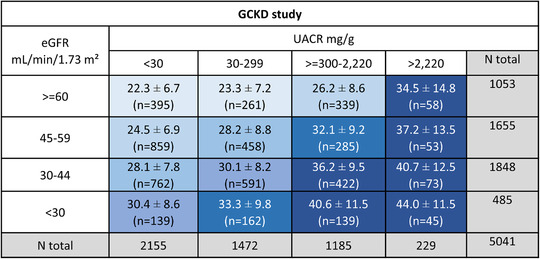
Methods: This was a prospective cohort study including 5141 Caucasian patients with available apoA-IV measurements and CKD. The majority of the patients had an estimated glomerular filtration rate (eGFR) of 30-60 ml/min/1.73m2 or an eGFR >60 ml/min/1.73m2 in the presence of overt proteinuria. Median follow-up was 6.5 years. The association of apoA-IV with comorbidities at baseline and endpoints during follow-up was modelled adjusting for major confounders.
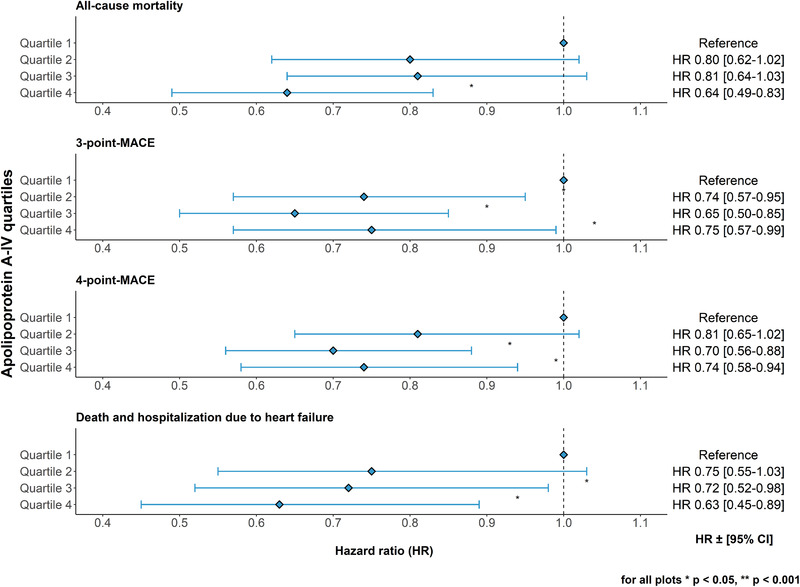
Results: Mean apoA-IV concentrations of the entire cohort were 28.9 ± 9.8 mg/dl. Patients in the highest apoA-IV quartile had the lowest high-sensitivity C-reactive protein values despite the highest prevalence of diabetes, albuminuria and the lowest eGFR. Each 10 mg/dl higher apoA-IV translated into lower odds of prevalent cardiovascular disease (1289 cases, odds ratio = 0.80, 95% confidence interval [CI] 0.72-0.86, p = 0.0000003). During follow-up, each 10 mg/dl higher apoA-IV was significantly associated with a lower risk for all-cause mortality (600 cases, hazard ratio [HR] = 0.81, 95% CI 0.73-0.89, p = 0.00004), incident major adverse cardiovascular events (506 cases, HR = 0.88, 95% CI 0.79-0.99, p = 0.03) and death or hospitalizations due to heart failure (346 cases, HR = 0.84, 95% CI 0.73-0.96, p = 0.01).
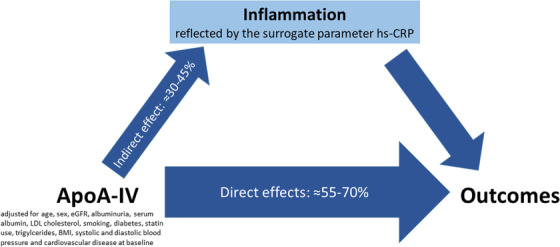
Conclusions: These data support a link between elevated apoA-IV concentrations and reduced inflammation in moderate CKD. ApoA-IV appears to be an independent risk marker for reduced all-cause mortality, cardiovascular events and heart failure in a large cohort of patients with CKD.
Keywords: all-cause mortality; apolipoprotein A-IV; cardiovascular disease; heart failure; high risk population; prospective study.
© 2021 The Authors. Journal of Internal Medicine published by John Wiley & Sons Ltd on behalf of Association for Publication of The Journal of Internal Medicine.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Eckardt K‐U, Coresh J, Devuyst O, Johnson RJ, Kottgen A, Levey AS, et al. Evolving importance of kidney disease: from subspecialty to global health burden. Lancet. 2013;382:158–69. - PubMed
-
- Jager KJ, Kovesdy C, Langham R, Rosenberg M, Jha V, Zoccali C. A single number for advocacy and communication‐worldwide more than 850 million individuals have kidney diseases. Nephrol Dial Transplant. 2019;34:1803–5. - PubMed
-
- Gansevoort RT, Correa‐Rotter R, Hemmelgarn BR, Jafar TH, Heerspink HJ, Mann JF, et al. Chronic kidney disease and cardiovascular risk: epidemiology, mechanisms, and prevention. Lancet. 2013;382:339–52. - PubMed
-
- Kronenberg F, Schernthaner GH. How many more data is required to give the kidney the attention it deserves? Time to act for the "big five" of cardiovascular risk. Atherosclerosis. 2020;297:146–8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
