

Geoeconomic variations in epidemiology, ventilation management, and outcomes in invasively ventilated intensive care unit patients without acute respiratory distress syndrome: a pooled analysis of four observational studies
- PMID: 34914899
- PMCID: PMC8766316
- DOI: 10.1016/S2214-109X(21)00485-X
Geoeconomic variations in epidemiology, ventilation management, and outcomes in invasively ventilated intensive care unit patients without acute respiratory distress syndrome: a pooled analysis of four observational studies
Abstract
Background: Geoeconomic variations in epidemiology, the practice of ventilation, and outcome in invasively ventilated intensive care unit (ICU) patients without acute respiratory distress syndrome (ARDS) remain unexplored. In this analysis we aim to address these gaps using individual patient data of four large observational studies.
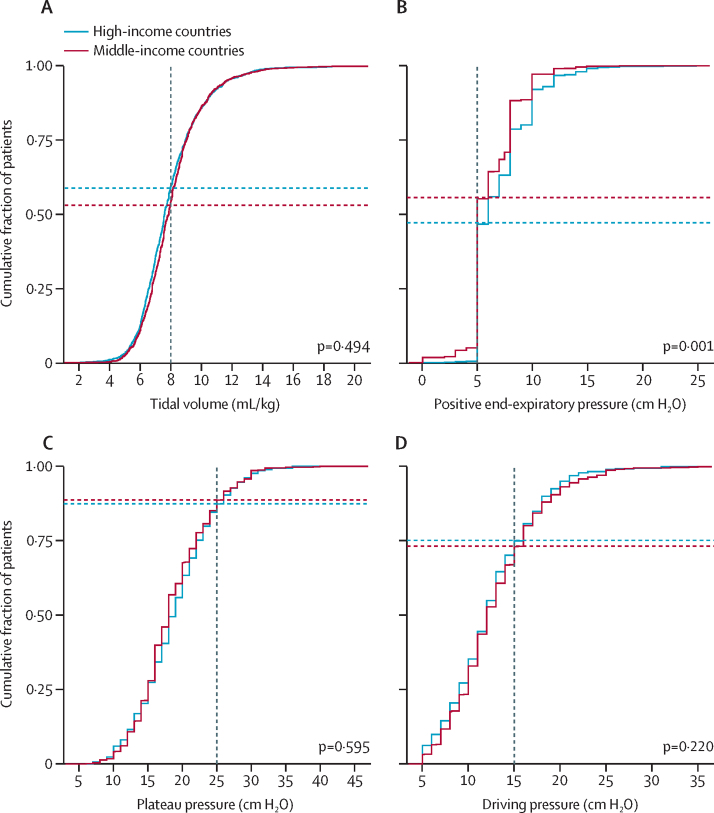
Methods: In this pooled analysis we harmonised individual patient data from the ERICC, LUNG SAFE, PRoVENT, and PRoVENT-iMiC prospective observational studies, which were conducted from June, 2011, to December, 2018, in 534 ICUs in 54 countries. We used the 2016 World Bank classification to define two geoeconomic regions: middle-income countries (MICs) and high-income countries (HICs). ARDS was defined according to the Berlin criteria. Descriptive statistics were used to compare patients in MICs versus HICs. The primary outcome was the use of low tidal volume ventilation (LTVV) for the first 3 days of mechanical ventilation. Secondary outcomes were key ventilation parameters (tidal volume size, positive end-expiratory pressure, fraction of inspired oxygen, peak pressure, plateau pressure, driving pressure, and respiratory rate), patient characteristics, the risk for and actual development of acute respiratory distress syndrome after the first day of ventilation, duration of ventilation, ICU length of stay, and ICU mortality.
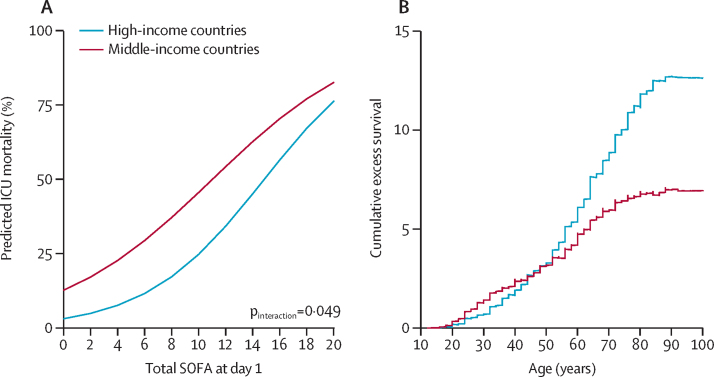
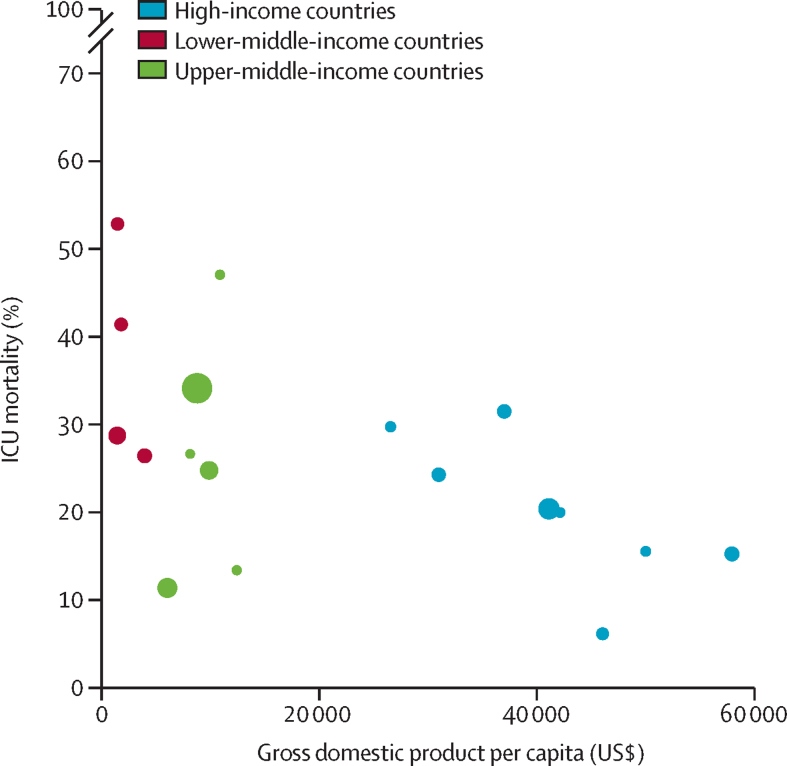
Findings: Of the 7608 patients included in the original studies, this analysis included 3852 patients without ARDS, of whom 2345 were from MICs and 1507 were from HICs. Patients in MICs were younger, shorter and with a slightly lower body-mass index, more often had diabetes and active cancer, but less often chronic obstructive pulmonary disease and heart failure than patients from HICs. Sequential organ failure assessment scores were similar in MICs and HICs. Use of LTVV in MICs and HICs was comparable (42·4% vs 44·2%; absolute difference -1·69 [-9·58 to 6·11] p=0·67; data available in 3174 [82%] of 3852 patients). The median applied positive end expiratory pressure was lower in MICs than in HICs (5 [IQR 5-8] vs 6 [5-8] cm H2O; p=0·0011). ICU mortality was higher in MICs than in HICs (30·5% vs 19·9%; p=0·0004; adjusted effect 16·41% [95% CI 9·52-23·52]; p<0·0001) and was inversely associated with gross domestic product (adjusted odds ratio for a US$10 000 increase per capita 0·80 [95% CI 0·75-0·86]; p<0·0001).
Interpretation: Despite similar disease severity and ventilation management, ICU mortality in patients without ARDS is higher in MICs than in HICs, with a strong association with country-level economic status.
Funding: No funding.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures
Comment in
-
Mortality in mechanically ventilated patients in middle-income countries: a call for action.Lancet Glob Health. 2022 Feb;10(2):e163-e164. doi: 10.1016/S2214-109X(21)00522-2. Epub 2021 Dec 13. Lancet Glob Health. 2022. PMID: 34914898 Free PMC article. No abstract available.
-
Improving the quality of intensive care in middle-income countries.Lancet Glob Health. 2022 Apr;10(4):e477-e478. doi: 10.1016/S2214-109X(22)00039-0. Lancet Glob Health. 2022. PMID: 35303454 No abstract available.
References
-
- Lalani HS, Waweru-Siika W, Mwogi T, et al. Intensive care outcomes and mortality prediction at a national referral hospital in western Kenya. Ann Am Thorac Soc. 2018;15:1336–1343. - PubMed
-
- Schultz MJ, Dunser MW, Dondorp AM, et al. Current challenges in the management of sepsis in ICUs in resource-poor settings and suggestions for the future. Intensive Care Med. 2017;43:612–624. - PubMed
-
- Riviello ED, Kiviri W, Twagirumugabe T, et al. Hospital incidence and outcomes of the acute respiratory distress syndrome using the Kigali modification of the Berlin definition. Am J Respir Crit Care Med. 2016;193:52–59. - PubMed
-
- Misango D, Pattnaik R, Baker T, Dünser MW, Dondorp AM, Schultz MJ. In: Sepsis management in resource-limited settings. Dondorp A, Dünser M, Schultz M, editors. Springer; Cham: 2019. Hemodynamic assessment and support in sepsis and septic shock in resource-limited settings; pp. 151–162. - PubMed
