

Exploring the implementation and underlying mechanisms of centralized referral systems to access specialized health services in Quebec
- PMID: 34915871
- PMCID: PMC8674406
- DOI: 10.1186/s12913-021-07286-3
Exploring the implementation and underlying mechanisms of centralized referral systems to access specialized health services in Quebec
Abstract
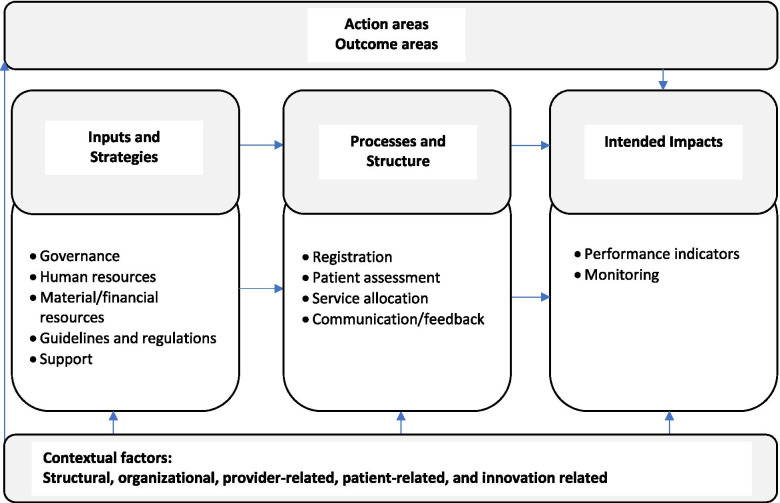
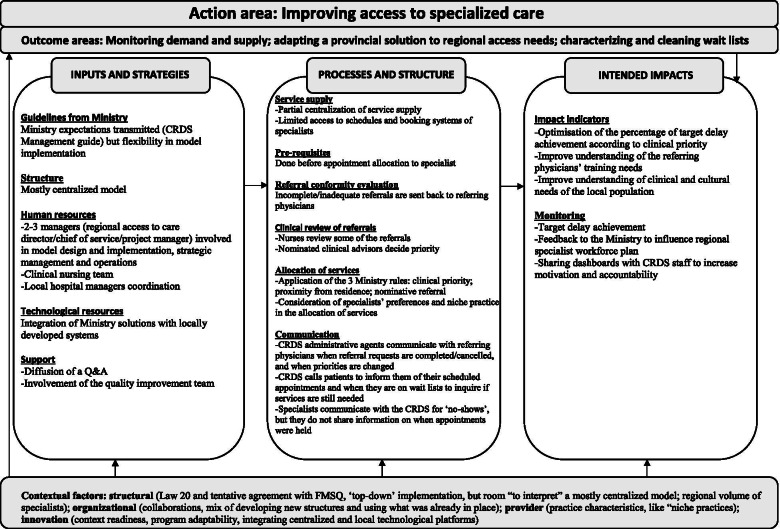
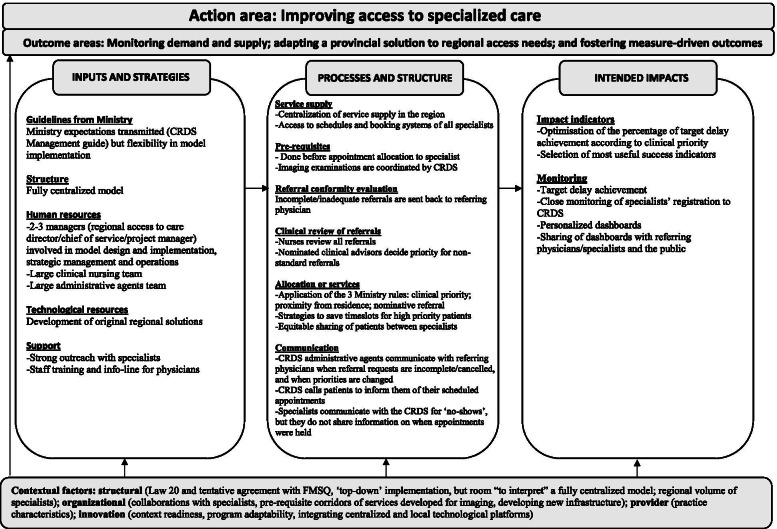
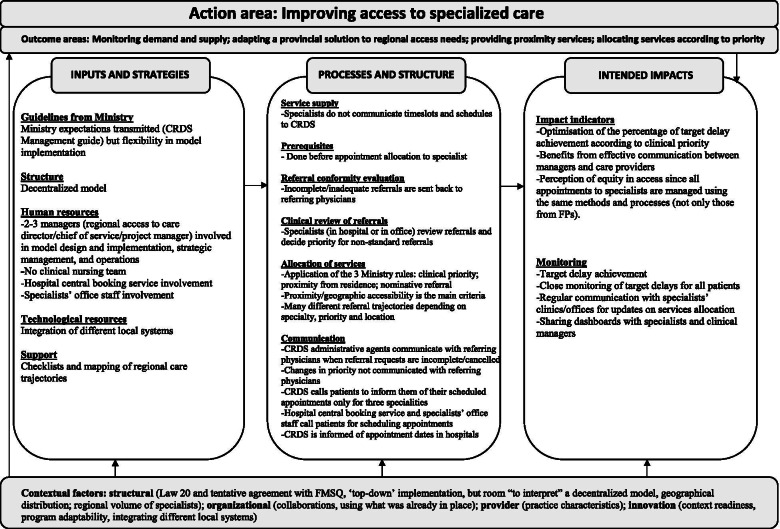
Background: In 2016, Quebec, a Canadian province, implemented a program to improve access to specialized health services (Accès priorisé aux services spécialisés (APSS)), which includes single regional access points for processing requests to such services via primary care (Centre de répartition des demandes de services (CRDS)). Family physicians fill out and submit requests for initial consultations with specialists using a standardized form with predefined prioritization levels according to listed reasons for consultations, which is then sent to the centralized referral system (the CRDS) where consultations with specialists are assigned. We 1) described the APSS-CRDS program in three Quebec regions using logic models; 2) compared similarities and differences in the components and processes of the APSS-CRDS models; and 3) explored contextual factors influencing the models' similarities and differences.
Methods: We relied on a qualitative study to develop logic models of the implemented APSS-CRDS program in three regions. Semi-structured interviews with health administrators (n = 9) were conducted. The interviews were analysed using a framework analysis approach according to the APSS-CRDS's components included in the initially designed program, Mitchell and Lewis (2003)'s logic model framework, and Chaudoir and colleagues (2013)'s framework on contextual factors' influence on an innovation's implementation.
Results: Findings show the APSS-CRDS program's regional variability in the implementation of its components, including its structure (centralized/decentralized), human resources involved in implementation and operation, processes to obtain specialists' availability and assess/relay requests, as well as monitoring methods. Variability may be explained by contextual factors' influence, like ministerial and medical associations' involvement, collaborations, the context's implementation readiness, physician practice characteristics, and the program's adaptability.
Interpretation: Findings are useful to inform decision-makers on the design of programs like the APSS-CRDS, which aim to improve access to specialists, the essential components for the design of these types of interventions, and how contextual factors may influence program implementation. Variability in program design is important to consider as it may influence anticipated effects, a next step for the research team. Results may also inform stakeholders should they wish to implement similar programs to increase access to specialized health services via primary care.
Keywords: Access to care; Centralized referral mechanisms; Health planning; Logic models; Quebec; Single-entry model; Specialized health services.
© 2021. The Author(s).
Conflict of interest statement
CS was involved in the implementation of the APSS-CRDS programme and is (at the time of writing this paper) employed by the Quebec Ministry of Health and Social Services to work on this programme. All other authors declare that they have no competing interests.
Figures
References
-
- Barua B, Jacques D, Collyer A. Waiting your turn: wait times for health care in Canada, 2018 report: The Fraser Institute; 2018. https://www.fraserinstitute.org/sites/default/files/waiting-your-turn-20.... Accessed 11 Aug 2020.
-
- Government of Canada . Canada’s health care system. 2016.
-
- Canadian Institute for Health Information . How Canada compares: results from the Commonwealth fund’s 2016 international health policy survey of adults in 11 countries — accessible report. 2017.
MeSH terms
LinkOut - more resources
Full Text Sources
