

Laparoscopic surgery produced less surgical smoke and contamination comparing with open surgery: the pilot study in fresh cadaveric experiment in COVID-19 pandemic
- PMID: 34915893
- PMCID: PMC8675110
- DOI: 10.1186/s12893-021-01432-8
Laparoscopic surgery produced less surgical smoke and contamination comparing with open surgery: the pilot study in fresh cadaveric experiment in COVID-19 pandemic
Abstract
Background: The SARS-CoV2 virus has been identified in abdominal cavity of the COVID-19 patients. Therefore, the potential viral transmission from any surgical created smoke in these patients is of concern especially in laparoscopic surgery. This study aimed to compare the amount of surgical smoke and surgical field contamination between laparoscopic and open surgery in fresh cadavers.
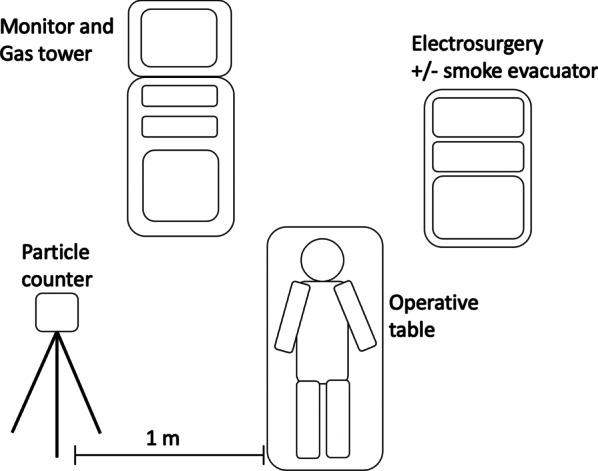
Methods: Cholecystectomy in 12 cadavers was performed and they were divided into 4 groups: laparoscopic approach with or without smoke evacuator, and open approach with or without smoke evacuator. The increased particle counts in surgical smoke of each group were analyzed. In the model of appendectomy, surgical field contamination under ultraviolet light and visual contamination scale between laparoscopic and open approach were compared.
Results: Open cholecystectomy significantly produced a greater amount of overall particle sizes, particle sizes < 5 μm and particle sizes ≥ 5 μm than laparoscopic cholecystectomy (10,307 × 103 vs 3738 × 103, 10,226 × 103 vs 3685 × 103 and 81 × 103 vs 53 × 103 count/m3, respectively at p < 0.05). The use of smoke evacuator led to decrease in the amount of overall particle sizes of 58% and 32.4% in the open and laparoscopic chelecystectomy respectively. Median (interquatile range) visual contamination scale of surgical field in open appendectomy [3.50 (2.33, 4.67)] was significantly greater than laparoscopic appendectomy [1.50 (0.67, 2.33)] at p < 0.001.
Conclusions: Laparoscopic cholecystectomy yielded less smoke-related particles than open cholecystectomy. The use of smoke evacuator, abeit non-significantly, reduced the particles in both open and laparoscopic cholecystectomy. Laparoscopic appendectomy had a lower degree of surgical field contamination than the open approach.
Keywords: COVID-19; Contamination; Laparoscopic surgery; Particle count; Smoke evacuator; Surgical smoke.
© 2021. The Author(s).
Conflict of interest statement
All authors declared there were no competing interests.
Figures



References
-
- Siegel JD, Rhinehart E, Jackson M, Chiarello L, Health Care Infection Control Practices Advisory C 2007 Guideline for isolation precautions: preventing transmission of infectious agents in health care settings. Am J Infect Control. 2007;35(102):S65–164. doi: 10.1016/j.ajic.2007.10.007. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
