

Goal-directed haemodynamic therapy during general anaesthesia for noncardiac surgery: a systematic review and meta-analysis
- PMID: 34916049
- PMCID: PMC8900265
- DOI: 10.1016/j.bja.2021.10.046
Goal-directed haemodynamic therapy during general anaesthesia for noncardiac surgery: a systematic review and meta-analysis
Abstract
Background: During general anaesthesia for noncardiac surgery, there remain knowledge gaps regarding the effect of goal-directed haemodynamic therapy on patient-centred outcomes.
Methods: Included clinical trials investigated goal-directed haemodynamic therapy during general anaesthesia in adults undergoing noncardiac surgery and reported at least one patient-centred postoperative outcome. PubMed and Embase were searched for relevant articles on March 8, 2021. Two investigators performed abstract screening, full-text review, data extraction, and bias assessment. The primary outcomes were mortality and hospital length of stay, whereas 15 postoperative complications were included based on availability. From a main pool of comparable trials, meta-analyses were performed on trials with homogenous outcome definitions. Certainty of evidence was evaluated using Grading of Recommendations, Assessment, Development, and Evaluations (GRADE).
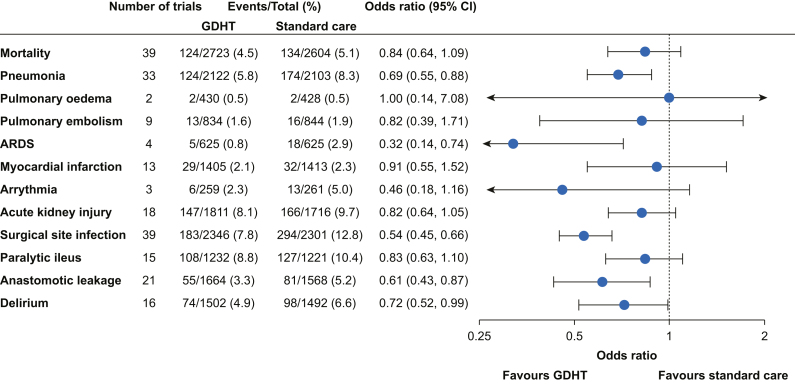
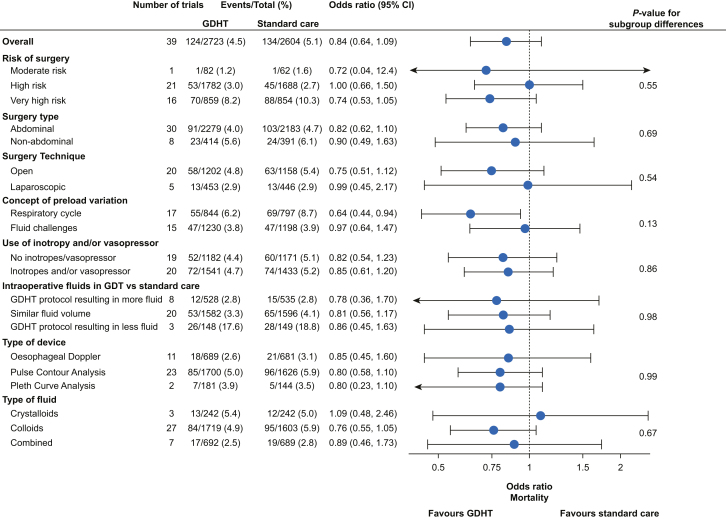
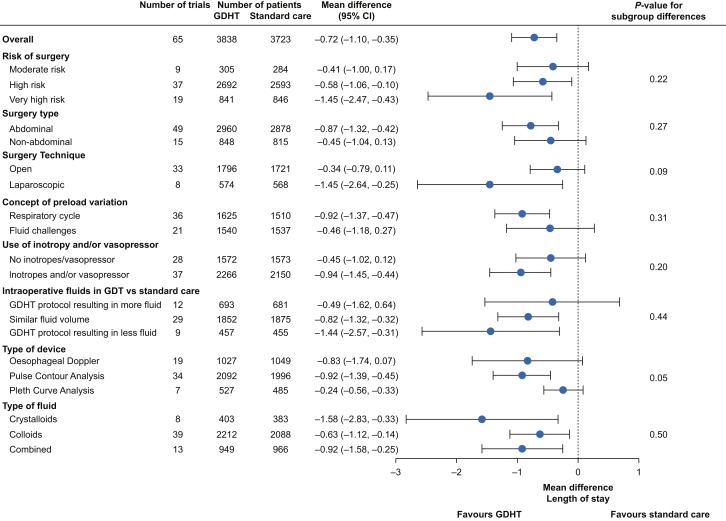
Results: The main pool consisted of 76 trials with intermediate risk of bias for most outcomes. Overall, goal-directed haemodynamic therapy might reduce mortality (odds ratio=0.84; 95% confidence interval [CI], 0.64 to 1.09) and shorten length of stay (mean difference=-0.72 days; 95% CI, -1.10 to -0.35) but with low certainty in the evidence. For both outcomes, larger effects favouring goal-directed haemodynamic therapy were seen in abdominal surgery, very high-risk surgery, and using targets based on preload variation by the respiratory cycle. However, formal tests for subgroup differences were not statistically significant. Goal-directed haemodynamic therapy decreased risk of several postoperative outcomes, but only infectious outcomes and anastomotic leakage reached moderate certainty of evidence.
Conclusions: Goal-directed haemodynamic therapy during general anaesthesia might decrease mortality, hospital length of stay, and several postoperative complications. Only infectious postoperative complications and anastomotic leakage reached moderate certainty in the evidence.
Keywords: fluid; general anaesthesia; goal-directed haemodynamic therapy; haemodynamics; perioperative care; postoperative complications; stroke volume.
Copyright © 2021 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
None of the authors have any conflicts of interests.
Figures
Comment in
-
Goal-directed haemodynamic therapy: what else? Comment on Br J Anaesth 2022; 128: 416-33.Br J Anaesth. 2022 Apr;128(4):e286-e288. doi: 10.1016/j.bja.2022.01.011. Epub 2022 Feb 5. Br J Anaesth. 2022. PMID: 35131095 No abstract available.
-
Goal-directed haemodynamic therapy: an imprecise umbrella term to avoid.Br J Anaesth. 2023 Apr;130(4):390-393. doi: 10.1016/j.bja.2022.12.022. Epub 2023 Jan 31. Br J Anaesth. 2023. PMID: 36732140
References
-
- Biccard B.M., Madiba T.E., Kluyts H.L., et al. Perioperative patient outcomes in the African Surgical Outcomes Study: a 7-day prospective observational cohort study. Lancet. 2018;391:1589–1598. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
