

SARS-CoV-2 vaccination and myocarditis or myopericarditis: population based cohort study
- PMID: 34916207
- PMCID: PMC8683843
- DOI: 10.1136/bmj-2021-068665
SARS-CoV-2 vaccination and myocarditis or myopericarditis: population based cohort study
Abstract
Objective: To investigate the association between SARS-CoV-2 vaccination and myocarditis or myopericarditis.
Design: Population based cohort study.
Setting: Denmark.
Participants: 4 931 775 individuals aged 12 years or older, followed from 1 October 2020 to 5 October 2021.
Main outcome measures: The primary outcome, myocarditis or myopericarditis, was defined as a combination of a hospital diagnosis of myocarditis or pericarditis, increased troponin levels, and a hospital stay lasting more than 24 hours. Follow-up time before vaccination was compared with follow-up time 0-28 days from the day of vaccination for both first and second doses, using Cox proportional hazards regression with age as an underlying timescale to estimate hazard ratios adjusted for sex, comorbidities, and other potential confounders.
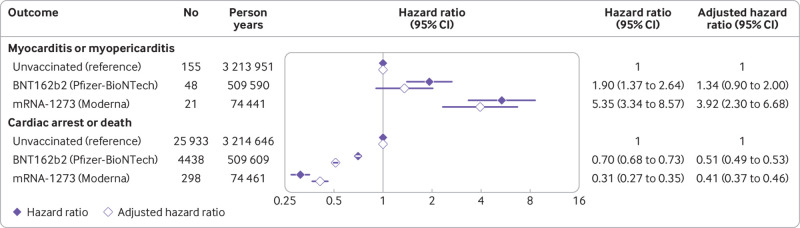
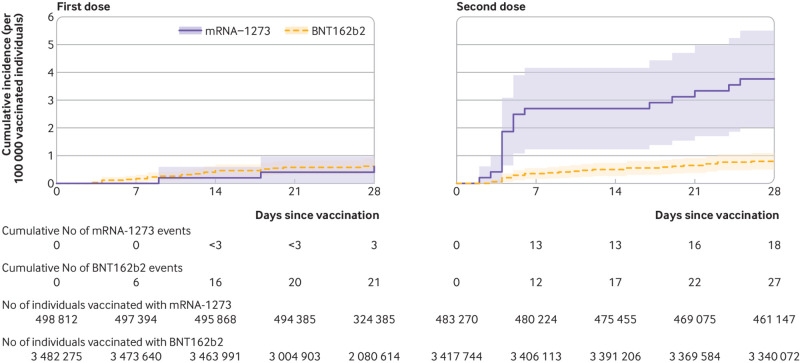
Results: During follow-up, 269 participants developed myocarditis or myopericarditis, of whom 108 (40%) were 12-39 years old and 196 (73%) were male. Of 3 482 295 individuals vaccinated with BNT162b2 (Pfizer-BioNTech), 48 developed myocarditis or myopericarditis within 28 days from the vaccination date compared with unvaccinated individuals (adjusted hazard ratio 1.34 (95% confidence interval 0.90 to 2.00); absolute rate 1.4 per 100 000 vaccinated individuals within 28 days of vaccination (95% confidence interval 1.0 to 1.8)). Adjusted hazard ratios among female participants only and male participants only were 3.73 (1.82 to 7.65) and 0.82 (0.50 to 1.34), respectively, with corresponding absolute rates of 1.3 (0.8 to 1.9) and 1.5 (1.0 to 2.2) per 100 000 vaccinated individuals within 28 days of vaccination, respectively. The adjusted hazard ratio among 12-39 year olds was 1.48 (0.74 to 2.98) and the absolute rate was 1.6 (1.0 to 2.6) per 100 000 vaccinated individuals within 28 days of vaccination. Among 498 814 individuals vaccinated with mRNA-1273 (Moderna), 21 developed myocarditis or myopericarditis within 28 days from vaccination date (adjusted hazard ratio 3.92 (2.30 to 6.68); absolute rate 4.2 per 100 000 vaccinated individuals within 28 days of vaccination (2.6 to 6.4)). Adjusted hazard ratios among women only and men only were 6.33 (2.11 to 18.96) and 3.22 (1.75 to 5.93), respectively, with corresponding absolute rates of 2.0 (0.7 to 4.8) and 6.3 (3.6 to 10.2) per 100 000 vaccinated individuals within 28 days of vaccination, respectively. The adjusted hazard ratio among 12-39 year olds was 5.24 (2.47 to 11.12) and the absolute rate was 5.7 (3.3 to 9.3) per 100 000 vaccinated individuals within 28 days of vaccination.
Conclusions: Vaccination with mRNA-1273 was associated with a significantly increased risk of myocarditis or myopericarditis in the Danish population, primarily driven by an increased risk among individuals aged 12-39 years, while BNT162b2 vaccination was only associated with a significantly increased risk among women. However, the absolute rate of myocarditis or myopericarditis after SARS-CoV-2 mRNA vaccination was low, even in younger age groups. The benefits of SARS-CoV-2 mRNA vaccination should be taken into account when interpreting these findings. Larger multinational studies are needed to further investigate the risks of myocarditis or myopericarditis after vaccination within smaller subgroups.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: support from the Lundbeck Foundation for the submitted work; MA declares that he has previously participated in research projects funded by Pfizer, Janssen, AstraZeneca, H Lundbeck and Mertz, and Novartis with grants received by Karolinska Institutet (no personal fees); MA has personally received fees for teaching from Atrium, the Danish Association of the Pharmaceutical Industry; the Pharmacovigilance Research Centre is supported by a grant from the Novo Nordisk Foundation (NNF15SA0018404) to the University of Copenhagen.
Figures

Comment in
-
Moderna COVID-19 vaccine was linked to myocarditis or myopericarditis at 28 d (4.2 events/100 000 persons).Ann Intern Med. 2022 May;175(5):JC58. doi: 10.7326/J22-0021. Epub 2022 May 3. Ann Intern Med. 2022. PMID: 35500266
References
-
- Shimabukuro T. COVID-19 Vaccine safety updates. Advisory Committee on Immunization Practices, 2021. https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-06/03-C....
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous