

Intrapleural nano-immunotherapy promotes innate and adaptive immune responses to enhance anti-PD-L1 therapy for malignant pleural effusion
- PMID: 34916656
- PMCID: PMC9074399
- DOI: 10.1038/s41565-021-01032-w
Intrapleural nano-immunotherapy promotes innate and adaptive immune responses to enhance anti-PD-L1 therapy for malignant pleural effusion
Abstract
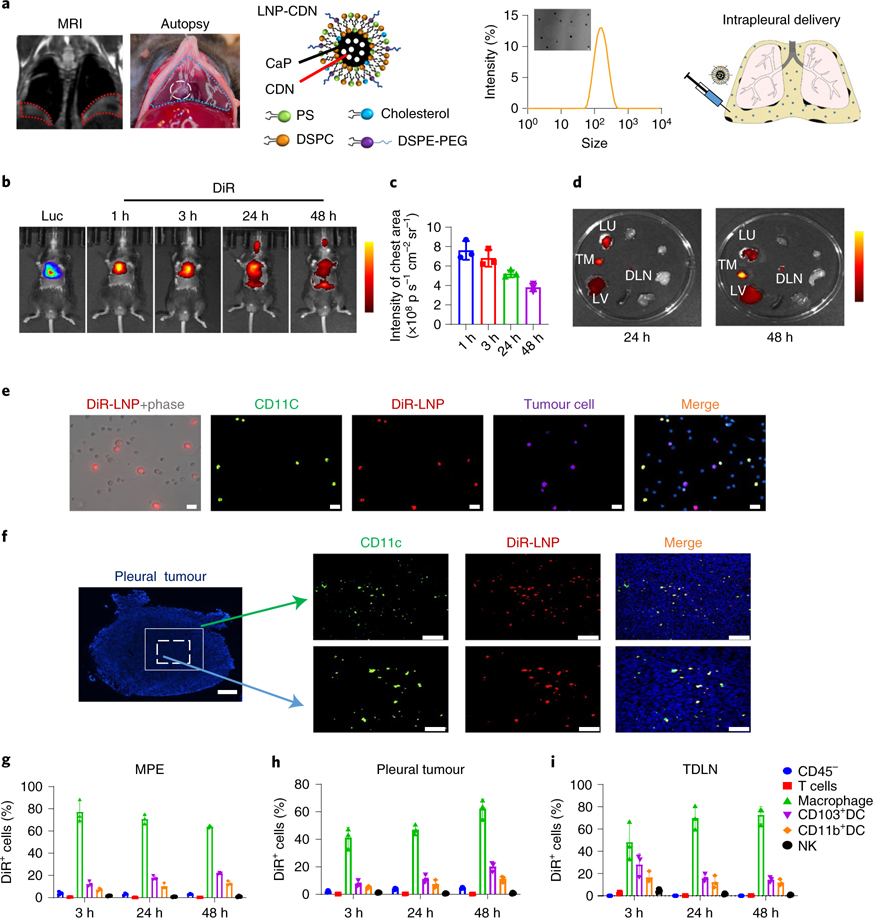
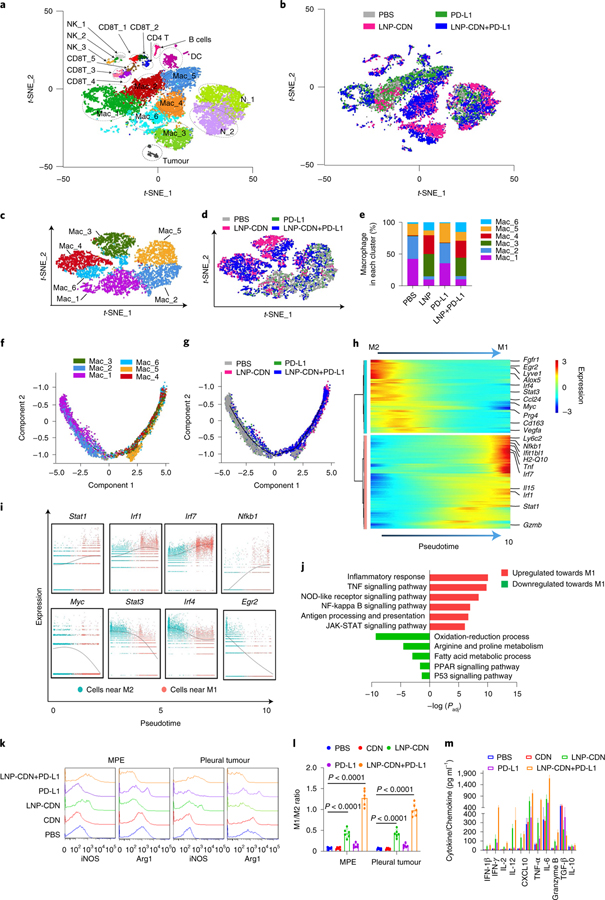
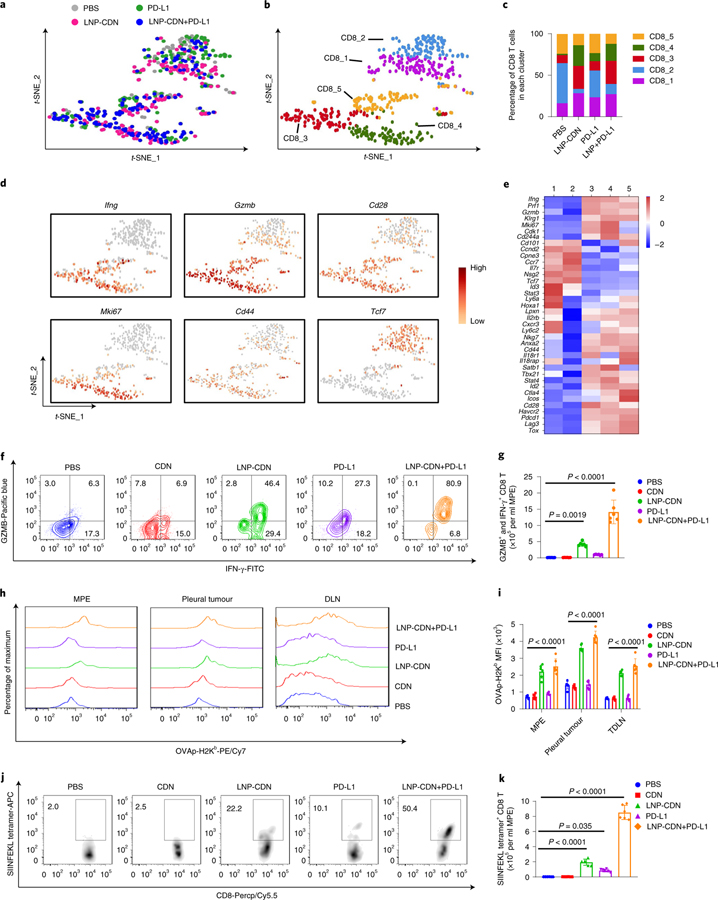
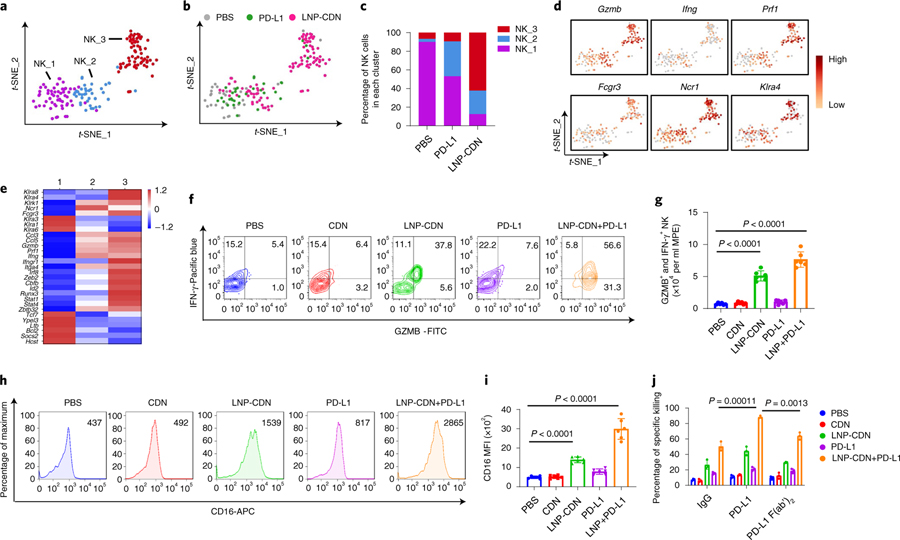
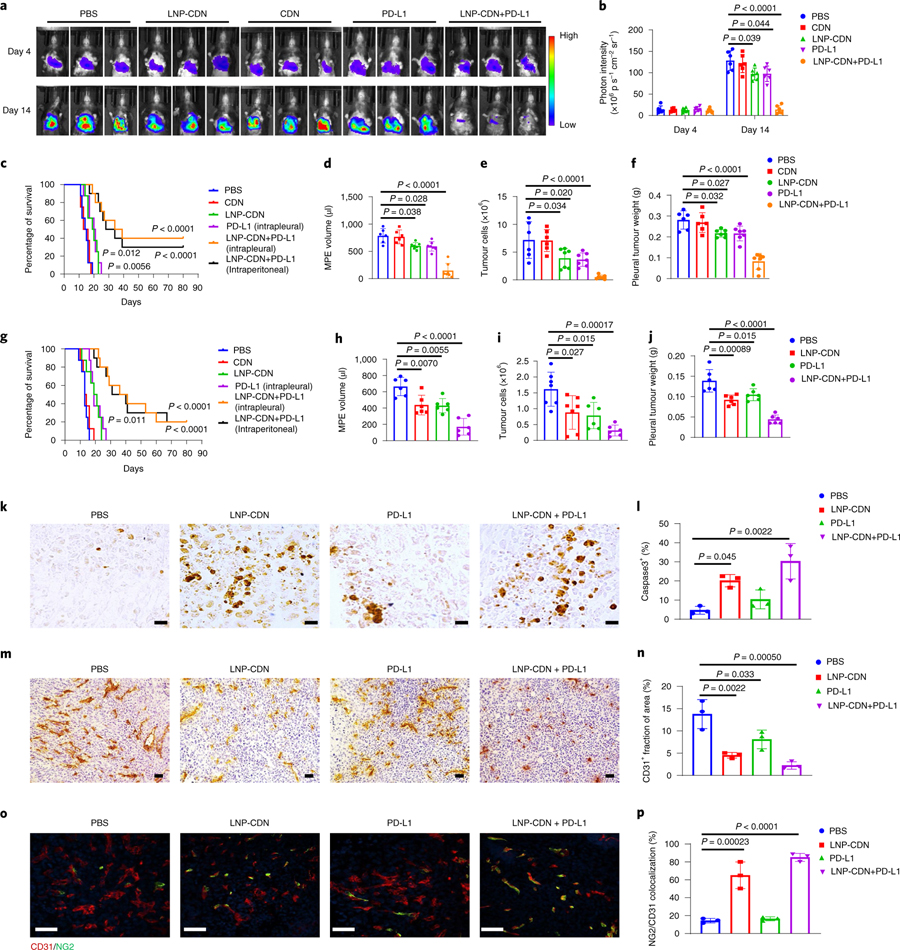
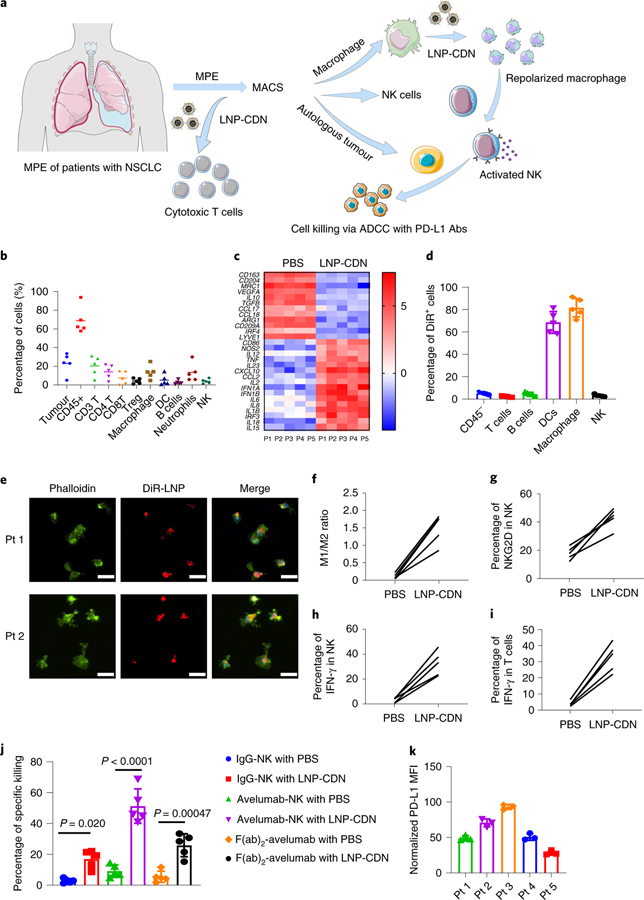
Malignant pleural effusion (MPE) is indicative of terminal malignancy with a uniformly fatal prognosis. Often, two distinct compartments of tumour microenvironment, the effusion and disseminated pleural tumours, co-exist in the pleural cavity, presenting a major challenge for therapeutic interventions and drug delivery. Clinical evidence suggests that MPE comprises abundant tumour-associated myeloid cells with the tumour-promoting phenotype, impairing antitumour immunity. Here we developed a liposomal nanoparticle loaded with cyclic dinucleotide (LNP-CDN) for targeted activation of stimulators of interferon genes signalling in macrophages and dendritic cells and showed that, on intrapleural administration, they induce drastic changes in the transcriptional landscape in MPE, mitigating the immune cold MPE in both effusion and pleural tumours. Moreover, combination immunotherapy with blockade of programmed death ligand 1 potently reduced MPE volume and inhibited tumour growth not only in the pleural cavity but also in the lung parenchyma, conferring significantly prolonged survival of MPE-bearing mice. Furthermore, the LNP-CDN-induced immunological effects were also observed with clinical MPE samples, suggesting the potential of intrapleural LNP-CDN for clinical MPE immunotherapy.
© 2021. The Author(s), under exclusive licence to Springer Nature Limited.
Conflict of interest statement
Competing interests
The authors declare no competing interests.
Figures
References
-
- Morgensztern D, Waqar S, Subramanian J, Trinkaus K & Govindan R Prognostic impact of malignant pleural effusion at presentation in patients with metastatic non-small-cell lung cancer. J. Thorac. Oncol. 7, 1485–1489 (2012). - PubMed
-
- American Thoracic Society. Management of malignant pleural effusions. Am. J. Respir. Crit. Care Med. 162, 1987–2001 (2000). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
