

Aminoglycoside- and glycopeptide-induced ototoxicity in children: a systematic review
- PMID: 34917943
- PMCID: PMC8669239
- DOI: 10.1093/jacamr/dlab184
Aminoglycoside- and glycopeptide-induced ototoxicity in children: a systematic review
Abstract
Background: Ototoxicity has been reported after administration of aminoglycosides and glycopeptides.
Objectives: To identify available evidence for the occurrence and determinants of aminoglycoside- and glycopeptide-related ototoxicity in children.
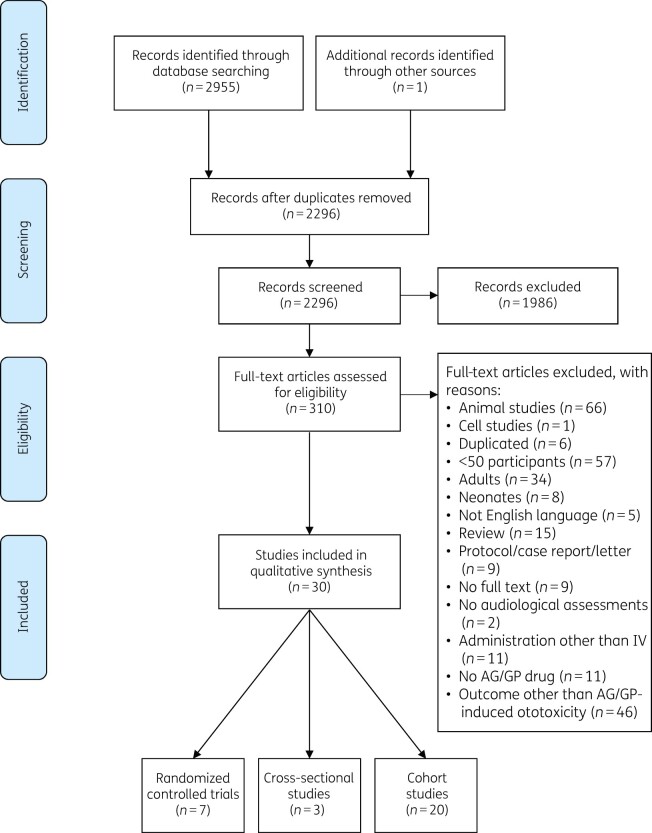
Materials and methods: Systematic electronic literature searches that combined ototoxicity (hearing loss, tinnitus and/or vertigo) with intravenous aminoglycoside and/or glycopeptide administration in children were performed in PubMed, EMBASE and Cochrane Library databases. Studies with sample sizes of ≥50 children were included. The QUIPS tool and Cochrane criteria were used to assess the quality and risk of bias of included studies.
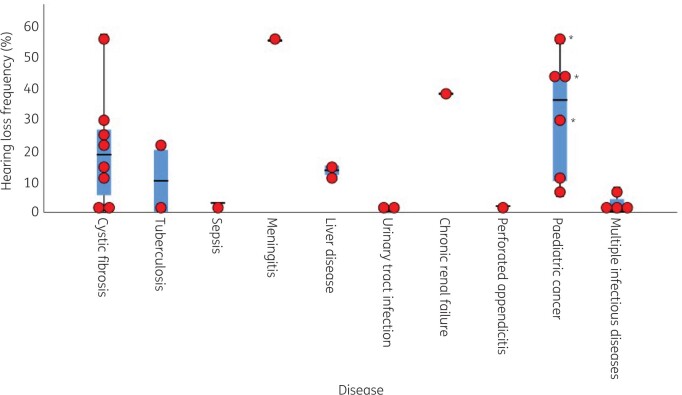
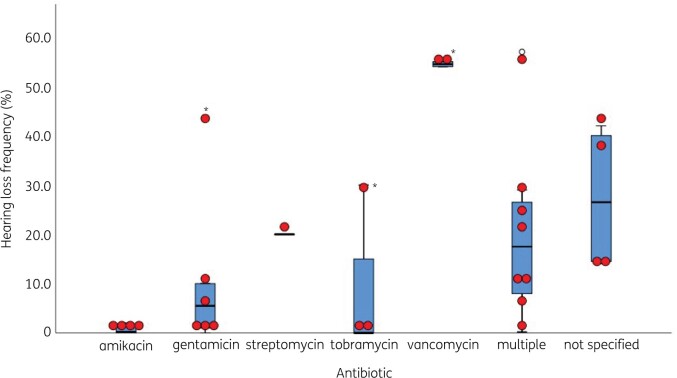
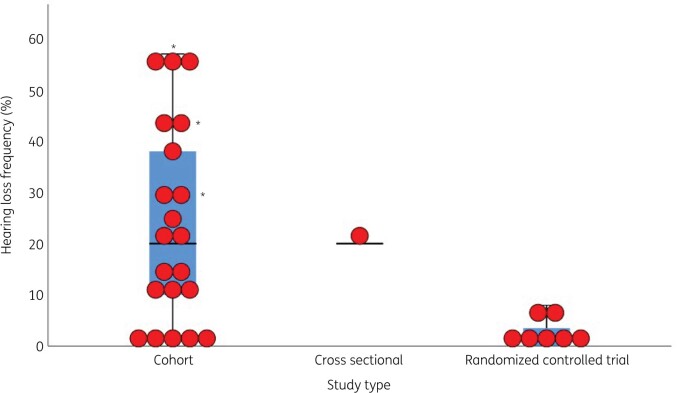
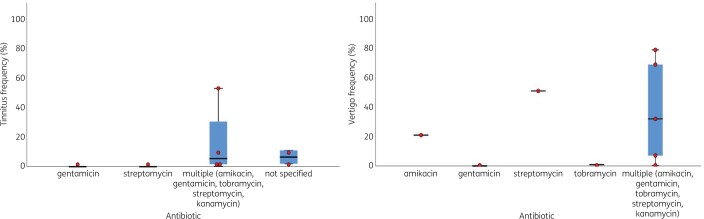
Results: Twenty-nine aminoglycoside-ototoxicity studies met the selection criteria (including 7 randomized controlled trials). Overall study quality was medium/low. The frequency of hearing loss within these studies ranged from 0%-57%, whereas the frequency of tinnitus and vertigo ranged between 0%-53% and 0%-79%, respectively. Two studies met the criteria on glycopeptide-induced ototoxicity and reported hearing loss frequencies of 54% and 55%. Hearing loss frequencies were higher in gentamicin-treated children compared to those treated with other aminoglycosides. In available studies aminoglycosides had most often been administered concomitantly with platinum agents, diuretics and other co-medication.
Conclusions: In children the reported occurrence of aminoglycoside/glycopeptide ototoxicity highly varies and seems to depend on the diagnosis, aminoglycoside subtype and use of co-administered medication. More research is needed to investigate the prevalence and determinants of aminoglycoside/glycopeptide ototoxicity. Our results indicate that age-dependent audiological examination may be considered for children frequently treated with aminoglycosides/glycopeptides especially if combined with other ototoxic medication.
© The Author(s) 2021. Published by Oxford University Press on behalf of the British Society for Antimicrobial Chemotherapy.
Figures
Similar articles
-
Extended-interval aminoglycoside administration for children: a meta-analysis.Pediatrics. 2004 Jul;114(1):e111-8. doi: 10.1542/peds.114.1.e111. Pediatrics. 2004. PMID: 15231982
-
A scoping review of global aminoglycoside antibiotic overuse: A potential opportunity for primary ototoxicity prevention.Res Social Adm Pharm. 2022 Aug;18(8):3220-3229. doi: 10.1016/j.sapharm.2021.10.004. Epub 2021 Oct 23. Res Social Adm Pharm. 2022. PMID: 34711521
-
Genetic susceptibility to aminoglycoside ototoxicity.Int J Pediatr Otorhinolaryngol. 2019 May;120:15-19. doi: 10.1016/j.ijporl.2019.02.002. Epub 2019 Feb 4. Int J Pediatr Otorhinolaryngol. 2019. PMID: 30743189
-
Intravenously delivered aminoglycoside antibiotics, tobramycin and amikacin, are not ototoxic in mice.Hear Res. 2020 Feb;386:107870. doi: 10.1016/j.heares.2019.107870. Epub 2019 Dec 13. Hear Res. 2020. PMID: 31864009
-
High-frequency audiometry reveals high prevalence of aminoglycoside ototoxicity in children with cystic fibrosis.J Cyst Fibros. 2015 Mar;14(2):248-54. doi: 10.1016/j.jcf.2014.07.009. Epub 2014 Aug 13. J Cyst Fibros. 2015. PMID: 25127922
Cited by
-
Drug-associated hearing impairment in children: a disproportionality analysis of the FDA adverse event reporting system.Front Pharmacol. 2025 Jun 26;16:1532461. doi: 10.3389/fphar.2025.1532461. eCollection 2025. Front Pharmacol. 2025. PMID: 40642015 Free PMC article.
-
Aminoglycosides-Related Ototoxicity: Mechanisms, Risk Factors, and Prevention in Pediatric Patients.Pharmaceuticals (Basel). 2023 Sep 25;16(10):1353. doi: 10.3390/ph16101353. Pharmaceuticals (Basel). 2023. PMID: 37895824 Free PMC article. Review.
-
Paediatric Escherichia coli urinary tract infection: susceptibility trends and clinical management-a retrospective analysis of a 10-year period.Ir J Med Sci. 2024 Aug;193(4):1891-1900. doi: 10.1007/s11845-024-03670-0. Epub 2024 Apr 3. Ir J Med Sci. 2024. PMID: 38565823
-
Maternal Exposure to Medications and the Risk of Congenital and Early-Onset Hearing Loss in Children: A Systematic Review and a Meta-Analysis.Basic Clin Pharmacol Toxicol. 2025 Sep;137(3):e70090. doi: 10.1111/bcpt.70090. Basic Clin Pharmacol Toxicol. 2025. PMID: 40851451 Free PMC article. Review.
-
Genetic Variations and Antibiotic-Related Adverse Events.Pharmaceuticals (Basel). 2024 Mar 2;17(3):331. doi: 10.3390/ph17030331. Pharmaceuticals (Basel). 2024. PMID: 38543117 Free PMC article. Review.
References
-
- Jackson J, Chen C, Buising K.. Aminoglycosides: how should we use them in the 21st century? Curr Opin Infect Dis 2013; 26: 516–25. - PubMed
-
- Poulikakos P, Falagas ME.. Aminoglycoside therapy in infectious diseases. Expert Opin Pharmacother 2013; 14: 1585–97. - PubMed
-
- Butler MS, Hansford KA, Blaskovich MAT. et al. Glycopeptide antibiotics: back to the future. J Antibiot (Tokyo) 2014; 67: 631–44. - PubMed
-
- de Jager P, van Altena R.. Hearing loss and nephrotoxicity in long-term aminoglycoside treatment in patients with tuberculosis. Int J Tuberc Lung Dis 2002; 6: 622–7. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous