

Evaluation of the association of length of stay in hospital and outcomes
- PMID: 34918090
- PMCID: PMC9070811
- DOI: 10.1093/intqhc/mzab160
Evaluation of the association of length of stay in hospital and outcomes
Abstract
Background: There exist wide variations in healthcare quality within the National Health Service (NHS). A shorter hospital length of stay (LOS) has been implicated as premature discharge, that may in turn lead to adverse consequences. We tested the hypothesis that a short LOS might be associated with increased risk of readmissions within 28 days of hospital discharge and also post-discharge mortality.
Methods: We conducted a single-centred study of 32 270 (46.1% men) consecutive alive-discharge episodes (mean age = 64.0 years, standard deviation = 20.5, range = 18-107 years), collected between 01/04/2017 and 31/03/2019. Associations of LOS tertiles (middle tertile as a reference) with readmissions and mortality were assessed using observed/expected ratios, and logistic and Cox regressions to estimate odds (OR) and hazard ratios (HR) (adjusted for age, sex, patients' severity of underlying health status and index admissions), with 95% confidence intervals (CIs).
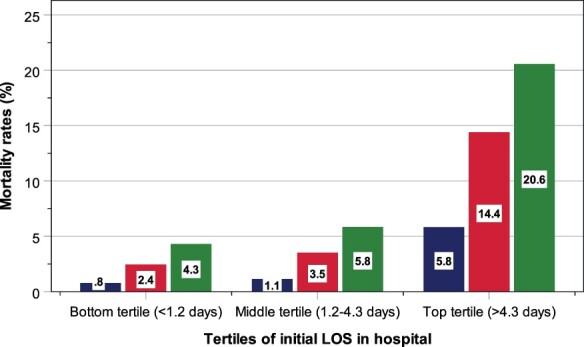
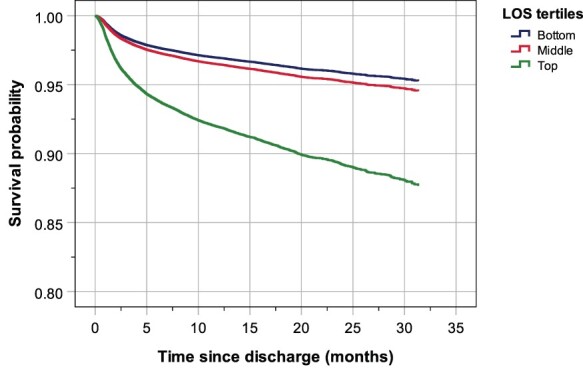
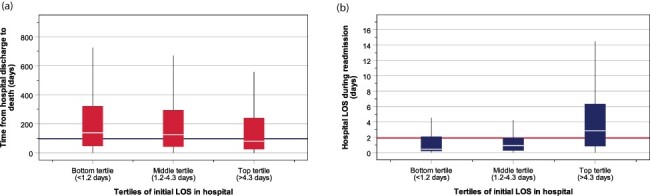
Results: The observed numbers of readmissions within 28 days of hospital discharge or post-discharge mortality were lower than expected (observed: expected ratio < 1) in patients in the bottom tertile (<1.2 days) and middle tertile (1.2-4.3 days) of LOS, whilst higher than expected (observed: expected ratio > 1) in patients in the top tertile (>4.3 days), amongst all ages. Patients in the top tertile of LOS had increased risks for one readmission: OR = 2.32 (95% CI = 1.86-2.88) or ≥2 readmissions: OR = 6.17 (95% CI = 5.11-7.45), death within 30 days: OR = 2.87 (95% CI = 2.34-3.51), and within six months of discharge: OR = 2.52 (95% CI = 2.23-2.85), and death over a two-year period: HR = 2.25 (95% CI = 2.05-2.47). The LOS explained 7.4% and 15.9% of the total variance (r2) in one readmission and ≥2 readmissions, and 9.1% and 10.0% of the total variance in mortality with 30 days and within six months of hospital discharge, respectively. Within the bottom, middle and top tertiles of the initial LOS, the median duration from hospital discharge to death progressively shortened from 136, 126 to 80 days, whilst LOS during readmission lengthened from 0.4, 0.9 to 2.8 days, respectively.
Conclusion: Short LOS in hospital was associated with favourable post-discharge outcomes such as early readmission and mortality, and with a delay in time interval from discharge to death and shorter LOS in hospital during readmission. These findings indicate that timely discharge from our hospital meets the aims of the NHS-generated national improvement programme, Getting It Right First Time.
Keywords: getting it right first time; health economy; measurement of quality; mortality; quality management.
© The Author(s) 2022. Published by Oxford University Press on behalf of International Society for Quality in Health Care.
Figures
References
-
- Inabnit LS, Blanchette C, Ruban C. Comorbidities and length of stay in chronic obstructive pulmonary disease patients. COPD 2018;15:355–60. - PubMed
-
- Anderson GF, Hussey PS. Population aging: a comparison among industrialized countries: populations around the world are growing older, but the trends are not cause for despair. Health Aff 2000;19:191–203. - PubMed
-
- Emergency Care Improvement Programme . Getting it Right In Emergency Care. https://gettingitrightfirsttime.co.uk/wp-content/uploads/2019/12/Getting... (9 May 2021, date last accessed).
-
- Abercrombie J. General Surgery: GIRFT Programme National Specialty Report. https://gettingitrightfirsttime.co.uk/wp-content/uploads/2017/07/GIRFT-G... (9 May 2021, date last accessed).
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
