

Diagnostic utility of CT for abdominal injury in the military setting: A systematic review and meta-analysis
- PMID: 34918669
- PMCID: PMC8677980
- DOI: 10.1097/MD.0000000000028150
Diagnostic utility of CT for abdominal injury in the military setting: A systematic review and meta-analysis
Abstract
Background: It is critical to accurately identify patients with abdominal injury who truly need to undergo laparotomy during the war in timely fashion. The diagnostic utility of computed tomography (CT) for evaluating abdominal injury in the military setting remains uncertain.
Methods: PubMed, EMBASE, and Cochrane Library databases were searched. Meta-analyses were performed by using a random-effect model. We pooled the area under the summary receiver operating characteristic curves with standard errors, the Q indexes with standard errors, the sensitivities with 95% confidence intervals (CIs), the specificities with 95% CIs, the positive likelihood ratios with 95% CIs, the negative likelihood ratios with 95% CIs, and the diagnostic odds ratios with 95% CIs. The heterogeneity among studies were evaluated by the I2 and P value.
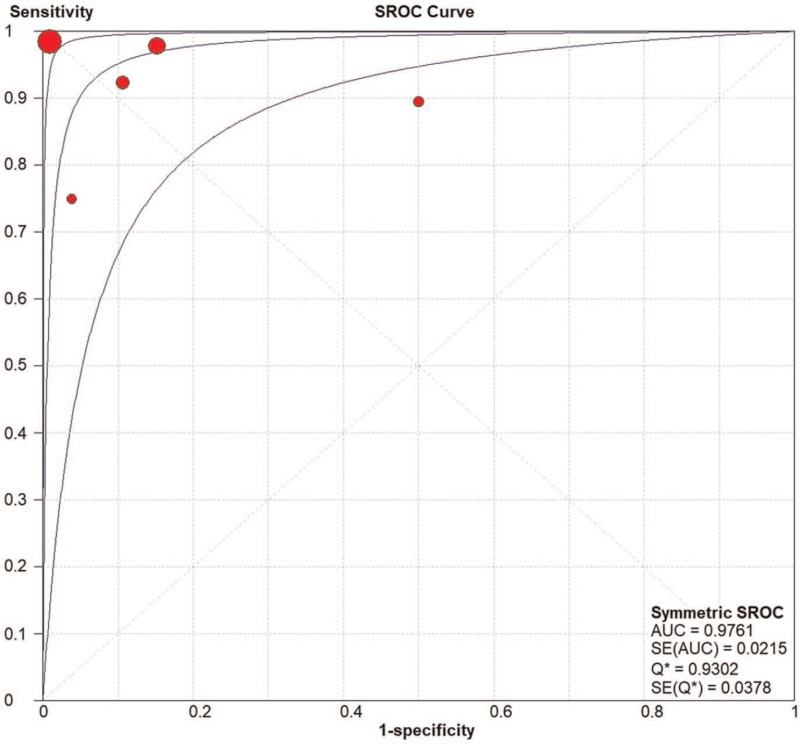
Results: Overall, 5 retrospective studies were included. The area under the summary receiver operating characteristic curve was 0.9761 ± 0.0215 and the Q index was 0.9302 ± 0.0378. The pooled sensitivity was 0.97 (95% CI = 0.92-0.99) without a significant heterogeneity among studies (I2 = 0%, P = .4538). The pooled specificity was 0.95 (95% CI = 0.93-0.97) with a significant heterogeneity among studies (I2 = 90.6%, P < .0001). The pooled positive likelihood ratio was 10.71 (95% CI: 2.91-39.43) with a significant heterogeneity among studies (I2 = 89.2%, P < .0001). The pooled negative likelihood ratio was 0.07 (95% CI = 0.02-0.27) with a significant heterogeneity among studies (I2 = 57.5%, P = .0516). The pooled diagnostic odds ratio was 177.48 (95% CI = 18.09-1741.31) with a significant heterogeneity among studies (I2 = 75.9%, P = .0023).
Conclusion: Diagnostic accuracy of CT for abdominal injury is excellent in the military setting. Further work should explore how to shrink CT equipment for a wider use in wartime.
Copyright © 2021 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures




References
-
- Moore EE, Moore JB, Van Duzer-Moore S, Thompson JS. Mandatory laparotomy for gunshot wounds penetrating the abdomen. Am J Surg 1980;140:847–51. - PubMed
-
- Demetriades D. Civilian and military trauma: training to successfully intervene and save lives. J Am Coll Surg 2018;227:555–63. - PubMed
-
- Sirinek KR, Page CP, Root HD, Levine BA. Is exploratory celiotomy necessary for all patients with truncal stab wounds? Arch Surg 1990;125:844–8. - PubMed
-
- Leppäniemi A, Salo J, Haapiainen R. Complications of negative laparotomy for truncal stab wounds. J Trauma 1995;38:54–8. - PubMed
-
- Miller FB, Cryer HM, Chilikuri S, Creech P, Richardson JD. Negative findings on laparotomy for trauma. South Med J 1989;82:1231–4. - PubMed
