

Diabetes and pre-diabetes in patients with heart failure and preserved ejection fraction
- PMID: 34918855
- PMCID: PMC9542636
- DOI: 10.1002/ejhf.2403
Diabetes and pre-diabetes in patients with heart failure and preserved ejection fraction
Abstract
Aim: There is an association between heart failure with preserved ejection fraction (HFpEF) and insulin resistance, but less is known about the diabetic continuum, and in particular about pre-diabetes, in HFpEF. We examined characteristics and outcomes of participants with diabetes or pre-diabetes in PARAGON-HF.
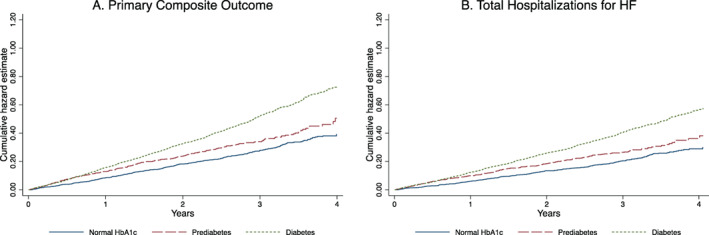
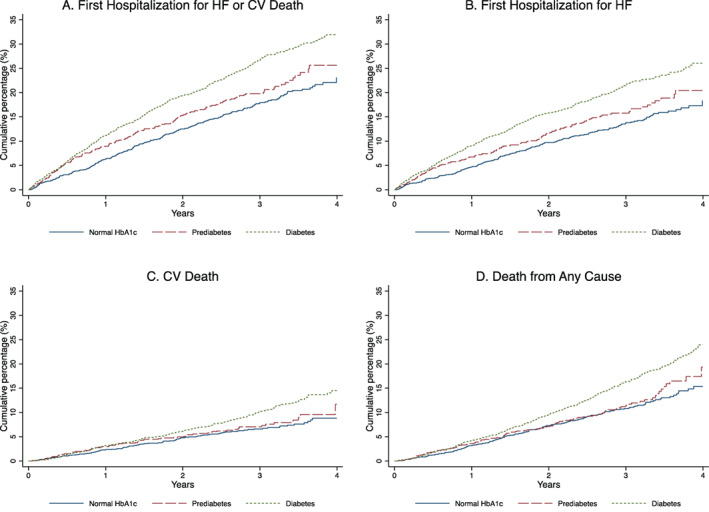
Methods and results: Patients aged ≥50 years with left ventricular ejection fraction ≥45%, structural heart disease and elevated N-terminal pro-B-type natriuretic peptide (NT-proBNP) were eligible. Patients were classified according to glycated haemoglobin (HbA1c): (i) normal HbA1c, <6.0%; (ii) pre-diabetes, 6.0%-6.4%; (iii) diabetes, ≥6.5% or history of diabetes. The primary outcome was a composite of cardiovascular (CV) death and total heart failure hospitalizations (HFH). Of 4796 patients, 50% had diabetes and 18% had pre-diabetes. Compared to patients with normal HbA1c, patients with pre-diabetes and diabetes more often were obese, had a history of myocardial infarction and had lower Kansas City Cardiomyopathy Questionnaire scores, while patients with diabetes had more clinical evidence of congestion, but similar NT-proBNP concentrations. The risks of the primary composite outcome (rate ratio [RR] 1.59, 95% confidence interval [CI] 1.35-1.88), total HFH (RR 1.67, 95% CI 1.39-2.02) and CV death (hazard ratio [HR] 1.35, 95% CI 1.07-1.71) were higher among patients with diabetes, compared to those with normal HbA1c. Patients with pre-diabetes had a higher risk (which was intermediate between that of patients with diabetes and those with normal HbA1c) of the primary outcome (HR 1.27, 95% CI 1.00-1.60) and HFH (HR 1.35, 95% CI 1.03-1.77), but not of CV death (HR 1.02, 95% CI 0.75-1.40). Patients with diabetes treated with insulin had worse outcomes than those not, and those with 'lean diabetes' had similar mortality rates to those with a higher body mass index, but lower rates of HFH.
Conclusion: Pre-diabetes is common in patients with HFpEF and is associated with worse clinical status and greater risk of HFH.
Clinical trial registration: ClinicalTrials.gov Identifier NCT01920711.
Keywords: Diabetes; Heart failure; Insulin; Obesity.
© 2021 The Authors. European Journal of Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Figures
Comment in
-
Diabesity and heart failure with preserved ejection fraction: the picture is getting clearer.Eur J Heart Fail. 2022 Mar;24(3):510-512. doi: 10.1002/ejhf.2440. Epub 2022 Feb 14. Eur J Heart Fail. 2022. PMID: 35118771 No abstract available.
References
-
- Khan SS, Butler J, Gheorghiade M. Management of comorbid diabetes mellitus and worsening heart failure. JAMA. 2014;311:2379–80. - PubMed
-
- Haffner S, Taegtmeyer H. Epidemic obesity and the metabolic syndrome. Circulation. 2003;108:1541–5. - PubMed
-
- Kannel WB, Hjortland M, Castelli WP. Role of diabetes in congestive heart failure: the Framingham study. Am J Cardiol. 1974;34:29–34. - PubMed
-
- MacDonald MR, Petrie MC, Varyani F, Ostergren J, Michelson EL, Young JB, et al.; CHARM Investigators. Impact of diabetes on outcomes in patients with low and preserved ejection fraction heart failure: an analysis of the Candesartan in Heart Failure: Assessment of Reduction in Mortality and morbidity (CHARM) programme. Eur Heart J. 2008;29:1377–85. - PubMed
-
- Huxley RR, Barzi F, Woo J, Giles G, Lam TH, Rahimi K, et al.; Asia Pacific Cohort Studies Collaboration. A comparison of risk factors for mortality from heart failure in Asian and non‐Asian populations: an overview of individual participant data from 32 prospective cohorts from the Asia‐Pacific region. BMC Cardiovasc Disord. 2014;14:61. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
