

Pharmacologically induced endolysosomal cholesterol imbalance through clinically licensed drugs itraconazole and fluoxetine impairs Ebola virus infection in vitro
- PMID: 34919035
- PMCID: PMC8745396
- DOI: 10.1080/22221751.2021.2020598
Pharmacologically induced endolysosomal cholesterol imbalance through clinically licensed drugs itraconazole and fluoxetine impairs Ebola virus infection in vitro
Abstract
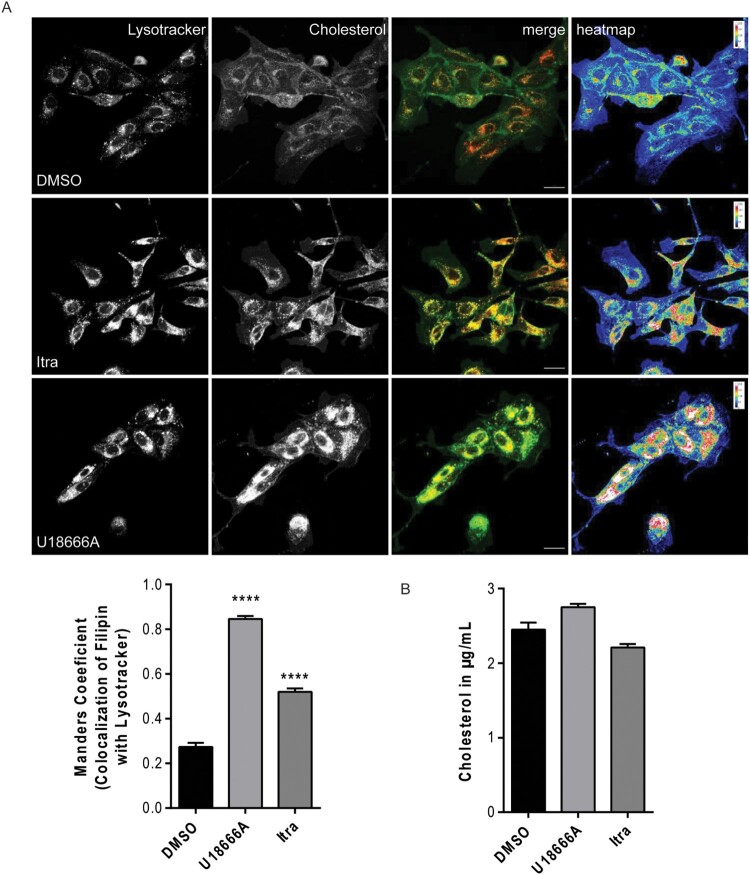
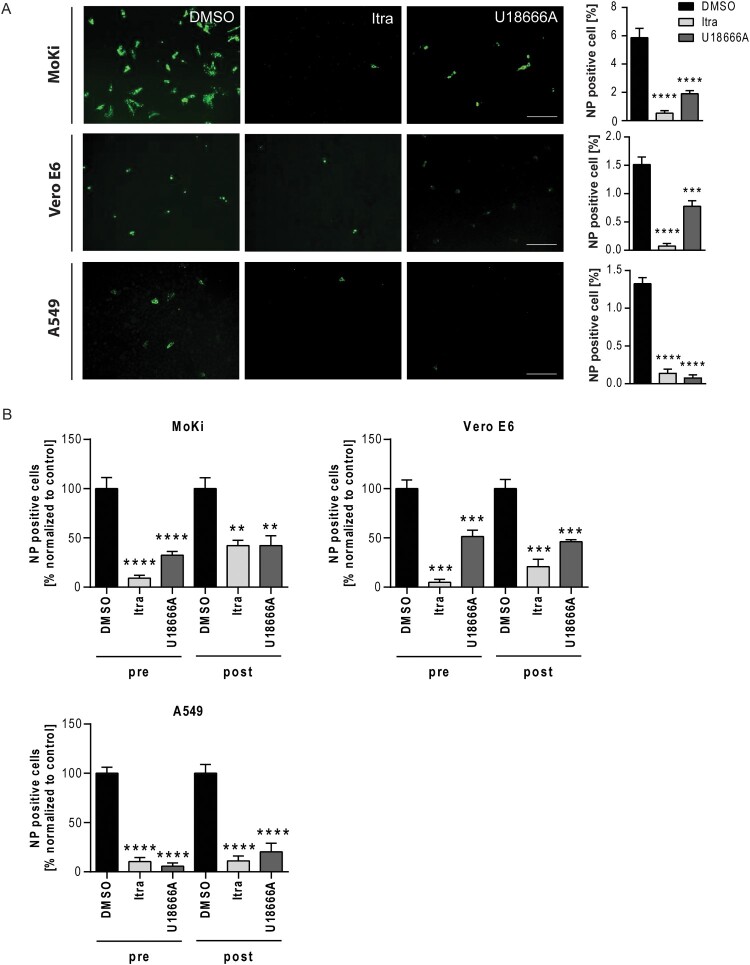
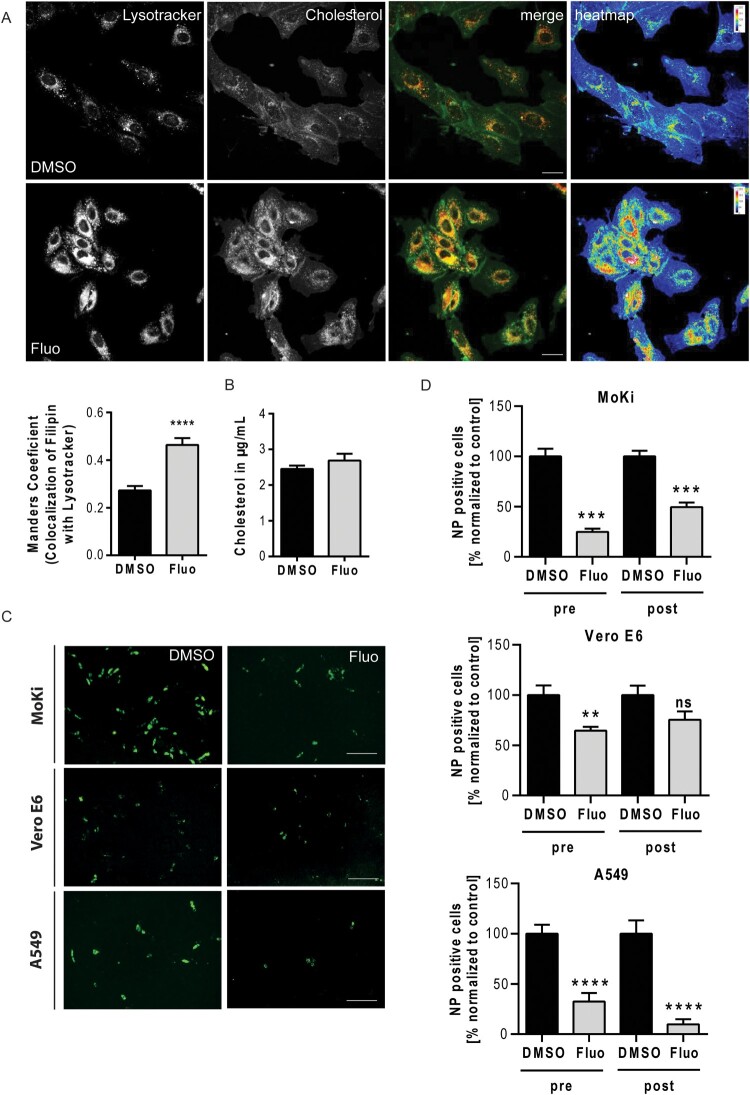
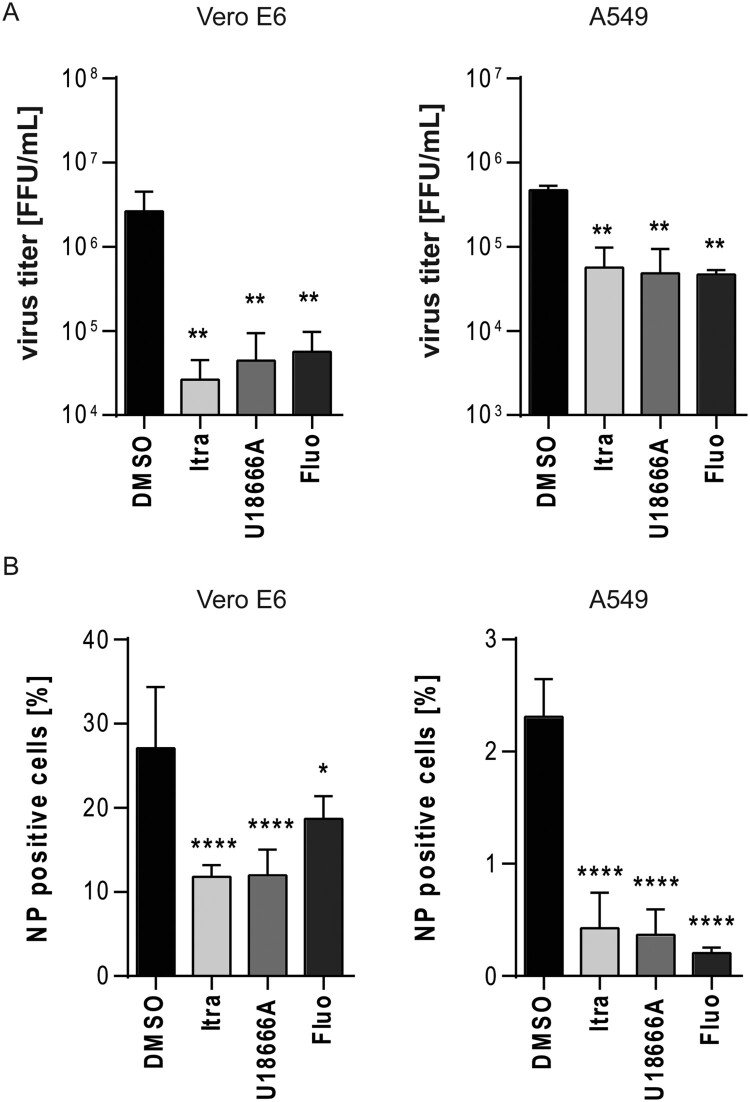
Ebola virus disease (EVD) is a severe and frequently lethal disease caused by Ebola virus (EBOV). The latest occasional EVD outbreak (2013-2016) in Western African, which was accompanied by a high fatality rate, showed the great potential of epidemic and pandemic spread. Antiviral therapies against EBOV are very limited, strain-dependent (only antibody therapies are available) and mostly restricted to symptomatic treatment, illustrating the urgent need for novel antiviral strategies. Thus, we evaluated the effect of the clinically widely used antifungal itraconazole and the antidepressant fluoxetine for a repurposing against EBOV infection. While itraconazole, similar to U18666A, directly binds to and inhibits the endosomal membrane protein Niemann-Pick C1 (NPC1), fluoxetine, which belongs to the structurally unrelated group of weakly basic, amphiphile so-called "functional inhibitors of acid sphingomyelinase" (FIASMA) indirectly acts on the lysosome-residing acid sphingomyelinase via enzyme detachment leading to subsequent lysosomal degradation. Both, the drug-induced endolysosomal cholesterol accumulation and the altered endolysosomal pH, might interfere with the fusion of viral and endolysosomal membrane, preventing infection with EBOV. We further provide evidence that cholesterol imbalance is a conserved cross-species mechanism to hamper EBOV infection. Thus, exploring the endolysosomal host-pathogen interface as a suitable antiviral treatment may offer a general strategy to combat EBOV infection.
Keywords: Ebola virus; FIASMA; Niemann-Pick C1; endolysosomal interference; fluoxetine; itraconazole; viral entry.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures
References
-
- World Health Organization . Ebola virus diease: key facts. Geneva: 2020.
-
- Ascenzi P, Bocedi A, Heptonstall J, et al. Ebolavirus and marburgvirus: insight the Filoviridae family. Mol Aspects Med. 2008;29(3):151–185. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical