

Association of Stage Shift and Population Mortality Among Patients With Non-Small Cell Lung Cancer
- PMID: 34919136
- PMCID: PMC8683966
- DOI: 10.1001/jamanetworkopen.2021.37508
Association of Stage Shift and Population Mortality Among Patients With Non-Small Cell Lung Cancer
Abstract
Importance: Early detection by computed tomography and a more attention-oriented approach to incidentally identified pulmonary nodules in the last decade has led to population stage shift for non-small cell lung cancer (NSCLC). This stage shift could substantially confound the evaluation of newer therapeutics and mortality outcomes.
Objective: To investigate the association of stage shift with population mortality among patients with NSCLC.
Design, setting, and participants: This retrospective cohort study was performed from October 2020 to June 2021 and used data from the Surveillance, Epidemiology, and End Results (SEER) registries to assess all patients from 2006 to 2016 with NSCLC.
Main outcomes and measures: Incidence-based mortality was evaluated by year-of-death. To assess shifts in diagnostic characteristics, clinical stage and histology distributions were examined by year using χ2 tests. Trends were assessed using the average annual percentage change (AAPC), calculated with JoinPoint software. Kaplan-Meier survival analysis assessed overall survival according to stage and compared those missing any stage with those with a reported stage.
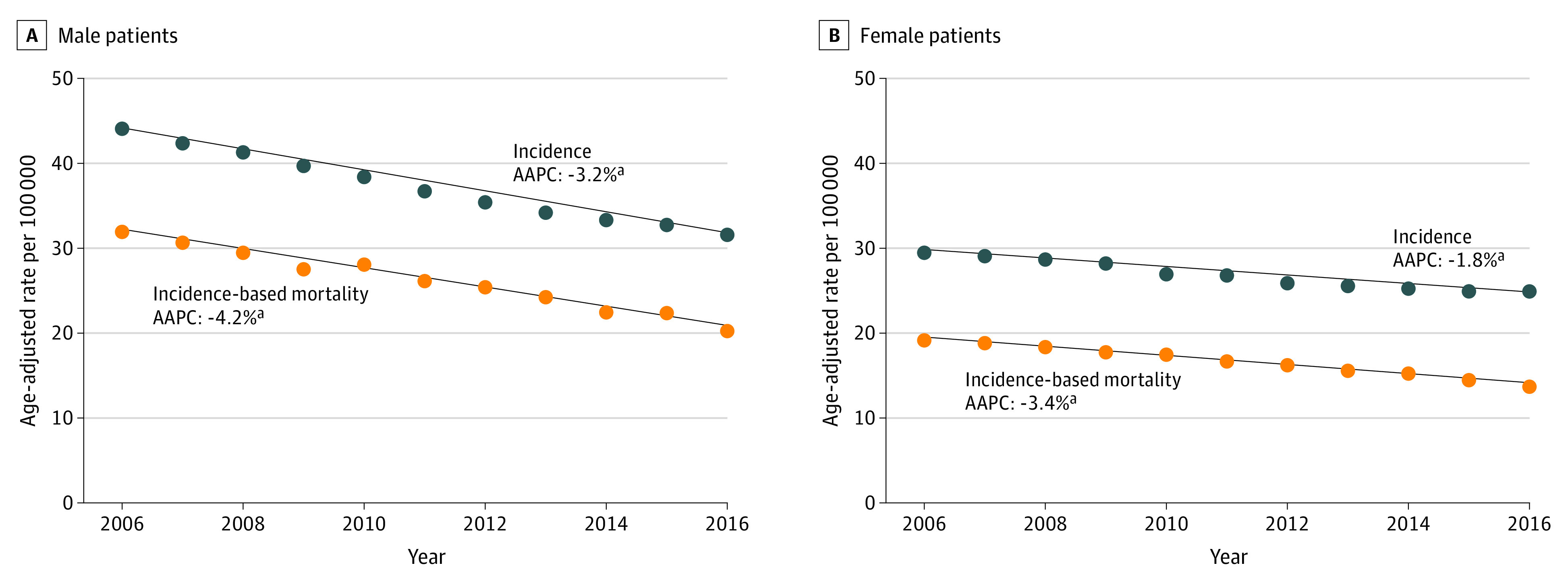
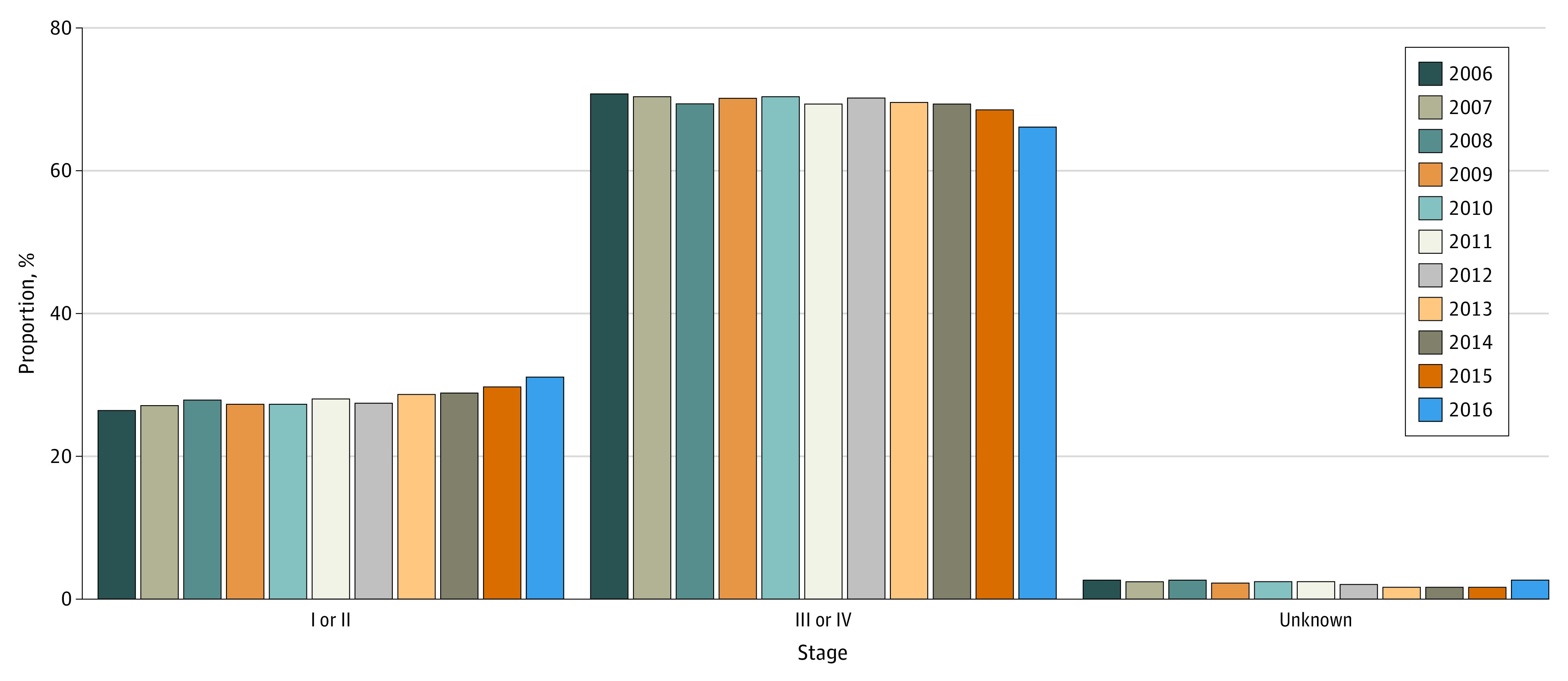
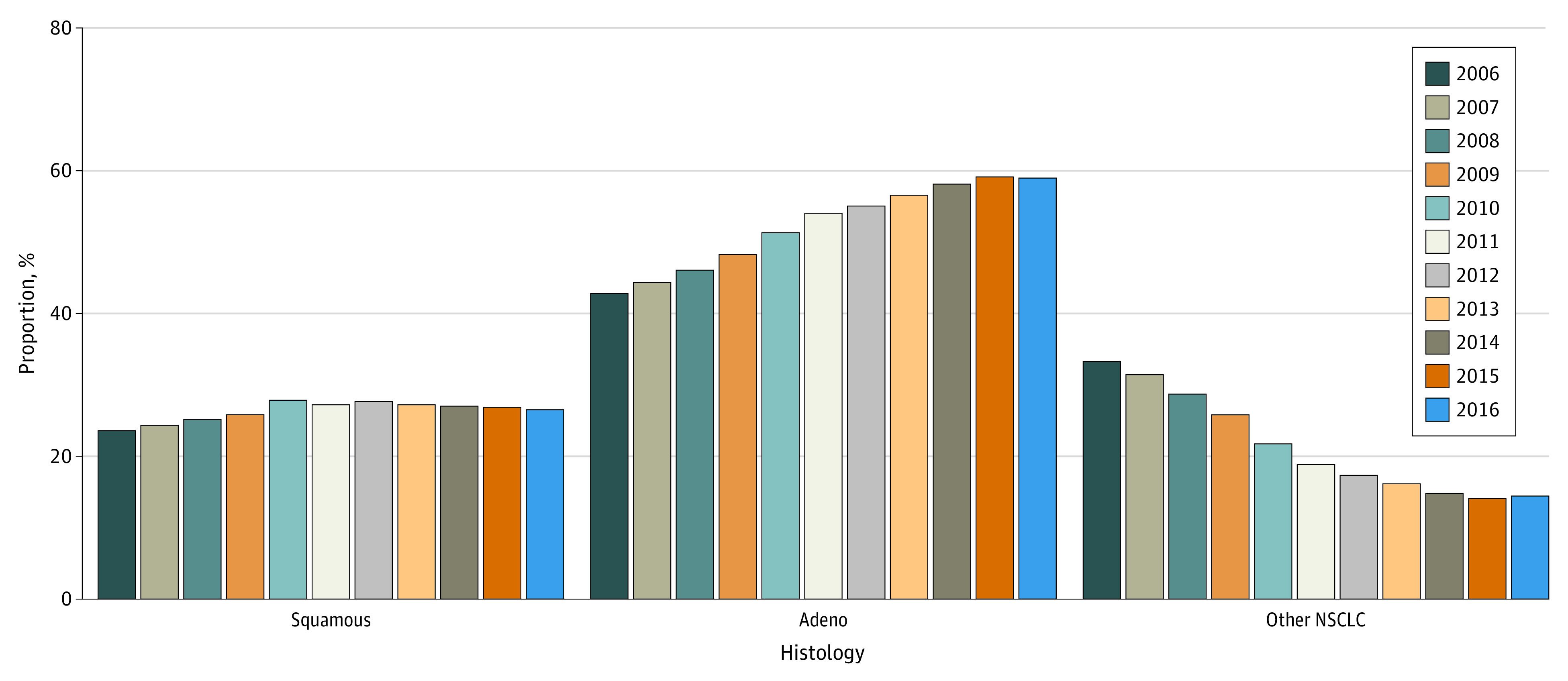
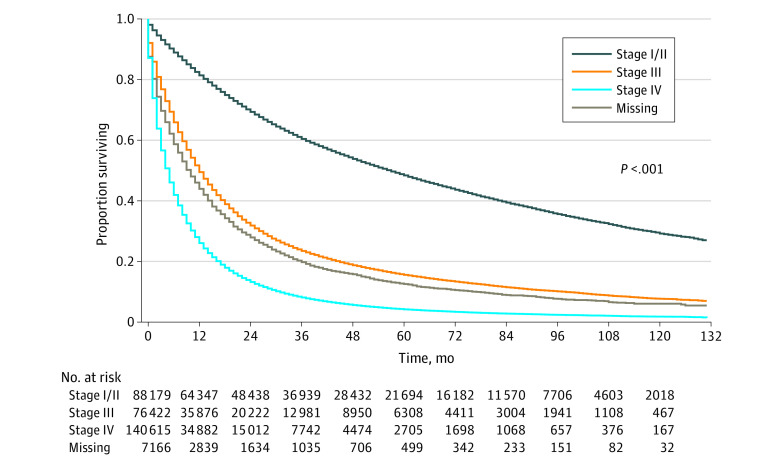
Results: The final sample contained 312 382 patients; 166 657 (53.4%) were male, 38 201 (12.2%) were Black, and 249 062 (79.7%) were White; the median (IQR) age was 68 (60-76) years; 163 086 (52.2%) had adenocarcinoma histology. Incidence-based mortality within 5 years of diagnosis decreased from 2006 to 2016 (AAPC, -3.7; 95% CI, -4.1 to -3.4). When assessing stage shift, there was significant association between year-of-diagnosis and clinical stage, with stage I/II diagnosis increasing from 26.5% to 31.2% (AAPC, 1.5; 95% CI, 0.5 to 2.5); and stage III/IV diagnosis decreasing significantly from 70.8% to 66.1% (AAPC, -0.6; 95% CI, -1.0 to -0.2). Missing staging information was not associated with year-of-diagnosis (AAPC, -1.6; 95% CI, -7.4 to 4.5). Year-of-diagnosis was significantly associated with tumor histology (χ2 = 8990.0; P < .001). There was a significant increase in adenocarcinomas: 42.9% in 2006 to 59.0% in 2016 (AAPC, 3.4; 95% CI, 2.9 to 3.9). Median (IQR) survival for stage I/II was 57 months (18 months to not reached); stage III/IV was 7 (2-19) months; and missing stage was 10 (2-28) months. When compared with those with known stage, those without stage information had significantly worse survival than those with stage I/II, with survival between those with stage III and stage IV (log-rank χ2 = 87 125.0; P < .001).
Conclusions and relevance: This cohort study found an association between decreased mortality and a corresponding diagnostic shift from later to earlier stage. These findings suggest that studies investigating the effect of treatment on lung cancer must take into account stage shift and the confounding association with survival and mortality outcome.
Conflict of interest statement
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
