

Detection of Pneumocystis jirovecii and Toxoplasma gondii in patients with lung infections by a duplex qPCR assay
- PMID: 34919557
- PMCID: PMC8682901
- DOI: 10.1371/journal.pntd.0010025
Detection of Pneumocystis jirovecii and Toxoplasma gondii in patients with lung infections by a duplex qPCR assay
Abstract
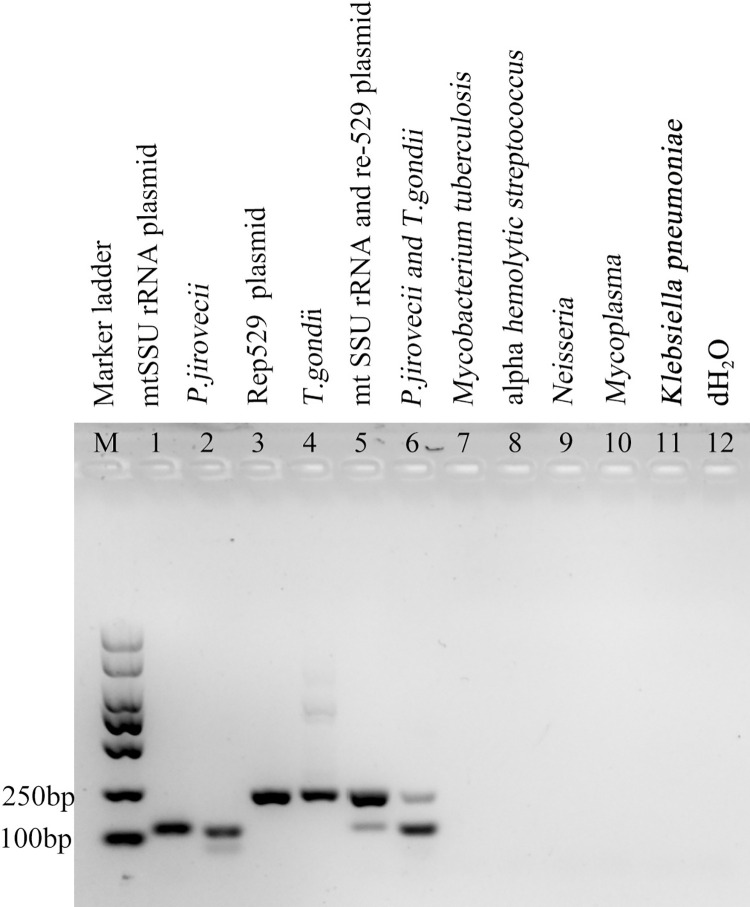
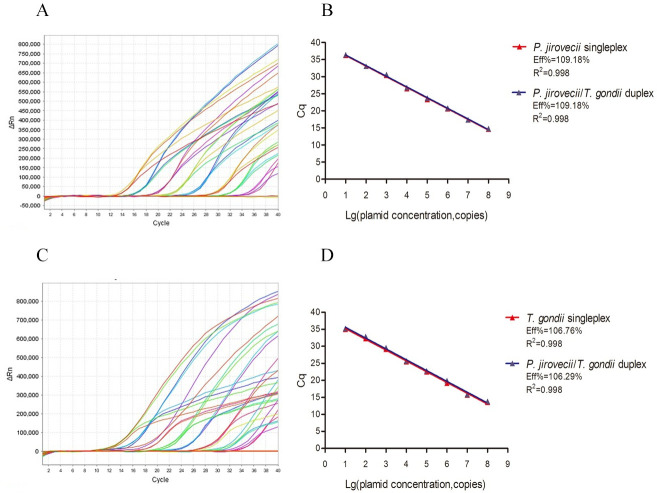
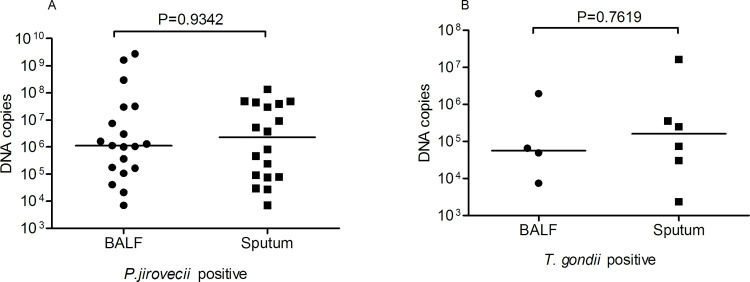
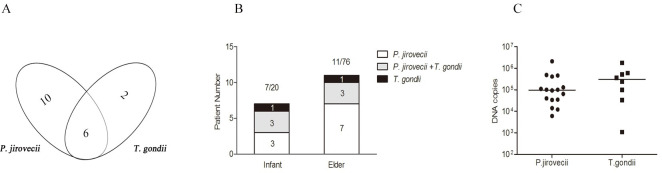
Pneumocystis pneumonia (PCP) and pulmonary toxoplasmosis (PT) are caused by Pneumocystis jirovecii and Toxoplasma gondii. The clinical symptoms and imaging of PCP and PT are indistinguishable. A duplex qPCR was developed to differentiate between these two pathogens. In testing 92 clinical samples to validate the performance of this method for P. jirovecii detection, it identified 31 positive samples for P. jirovecii infection, consistent with clinical diagnosis. Among the remainder of the 61 clinical samples with suspected PCP, yet showing as negative by the conventional PCR diagnosis approach, 6 of them proved positive using our new assay. Our new approach also produced similar results in identification of T. gondii infections, giving a result of 2 positive and 20 negative in clinical samples. An investigation was undertaken on the prevalence of P. jirovecii and T. gondii infections using 113 samples from lung infection patients. 9% (10/113) were shown to be positive with infections of P. jirovecii, 2% with T. gondii (2/113) and 5% (6/113) were co-infected with both pathogens. Although this duplex qPCR can detect individual P. jirovecii and T. gondii infection, and co-infection of both pathogens, further large-scale investigations are needed to validate its performance, especially in T. gondii detection. Our assay provides a rapid and accurate tool for PCP and PT diagnosis in immunocompromised population and clinical surveillance of these infections in patients with no immune defects.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Combined quantification of pulmonary Pneumocystis jirovecii DNA and serum (1->3)-β-D-glucan for differential diagnosis of pneumocystis pneumonia and Pneumocystis colonization.J Clin Microbiol. 2013 Oct;51(10):3380-8. doi: 10.1128/JCM.01554-13. Epub 2013 Jul 31. J Clin Microbiol. 2013. PMID: 23903553 Free PMC article.
-
[Investigation of Pneumocystis jirovecii pneumonia and colonization in iatrogenically immunosuppressed and immunocompetent patients].Mikrobiyol Bul. 2015 Apr;49(2):221-30. doi: 10.5578/mb.9344. Mikrobiyol Bul. 2015. PMID: 26167822 Turkish.
-
Real-time PCR assay-based strategy for differentiation between active Pneumocystis jirovecii pneumonia and colonization in immunocompromised patients.Clin Microbiol Infect. 2011 Oct;17(10):1531-7. doi: 10.1111/j.1469-0691.2010.03400.x. Epub 2011 Apr 12. Clin Microbiol Infect. 2011. PMID: 20946413
-
Recent Advances in the Diagnosis of Pneumocystis Pneumonia.Med Mycol J. 2016;57(4):E111-E116. doi: 10.3314/mmj.16-00019. Med Mycol J. 2016. PMID: 27904052 Review.
-
Clinical, Diagnostic, and Treatment Disparities between HIV-Infected and Non-HIV-Infected Immunocompromised Patients with Pneumocystis jirovecii Pneumonia.Respiration. 2018;96(1):52-65. doi: 10.1159/000487713. Epub 2018 Apr 10. Respiration. 2018. PMID: 29635251 Review.
Cited by
-
Evaluation of the Performance of a Multiplex Real-Time PCR Assay for the Identification of Aspergillus, Cryptococcus neoformans, and Pneumocystis jirovecii Simultaneously from Sputum in Multicenter [Letter].Infect Drug Resist. 2022 Nov 24;15:6799-6800. doi: 10.2147/IDR.S396184. eCollection 2022. Infect Drug Resist. 2022. PMID: 36451899 Free PMC article. No abstract available.
-
Establishment of an RPA-CRISPR/Cas12a combined diagnostic system for Pneumocystis jirovecii pneumonia.PLoS Negl Trop Dis. 2025 Mar 18;19(3):e0012922. doi: 10.1371/journal.pntd.0012922. eCollection 2025 Mar. PLoS Negl Trop Dis. 2025. PMID: 40100800 Free PMC article.
-
Toxoplasma gondii microneme protein MIC3 induces macrophage TNF-α production and Ly6C expression via TLR11/MyD88 pathway.PLoS Negl Trop Dis. 2023 Feb 2;17(2):e0011105. doi: 10.1371/journal.pntd.0011105. eCollection 2023 Feb. PLoS Negl Trop Dis. 2023. PMID: 36730424 Free PMC article.
-
Coinfection of Toxoplasma gondii and Other Microorganisms: A Systematic Review and Meta-Analysis.Microorganisms. 2024 Oct 21;12(10):2106. doi: 10.3390/microorganisms12102106. Microorganisms. 2024. PMID: 39458415 Free PMC article.
-
Analysis of Mutations in Pneumocystis jirovecii Dihydropteroate Synthase and Dihydropteroate Reductase Genes Among Non-HIV Patients in China.Infect Drug Resist. 2024 Dec 17;17:5619-5627. doi: 10.2147/IDR.S491478. eCollection 2024. Infect Drug Resist. 2024. PMID: 39711828 Free PMC article.
References
-
- Alanio A, Hauser PM, Lagrou K, Melchers WJ, Helweg-Larsen J, Matos O, et al.. ECIL guidelines for the diagnosis of Pneumocystis jirovecii pneumonia in patients with haematological malignancies and stem cell transplant recipients. J Antimicrob Chemother. 2016;71(9):2386–96. doi: 10.1093/jac/dkw156 . - DOI - PubMed
-
- Conrad A, Le Marechal M, Dupont D, Ducastelle-Lepretre S, Balsat M, Labussiere-Wallet H, et al.. A matched case-control study of toxoplasmosis after allogeneic haematopoietic stem cell transplantation: still a devastating complication. Clin Microbiol Infect. 2016;22(7):636–41. doi: 10.1016/j.cmi.2016.04.025 . - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
