

Neuronal synchrony abnormalities associated with subclinical epileptiform activity in early-onset Alzheimer's disease
- PMID: 34919638
- PMCID: PMC9630715
- DOI: 10.1093/brain/awab442
Neuronal synchrony abnormalities associated with subclinical epileptiform activity in early-onset Alzheimer's disease
Abstract
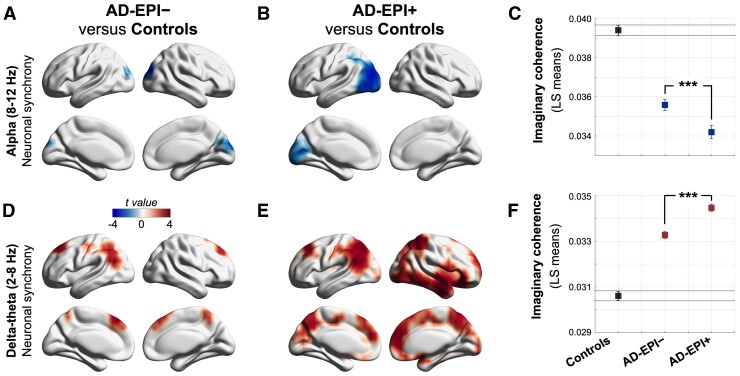
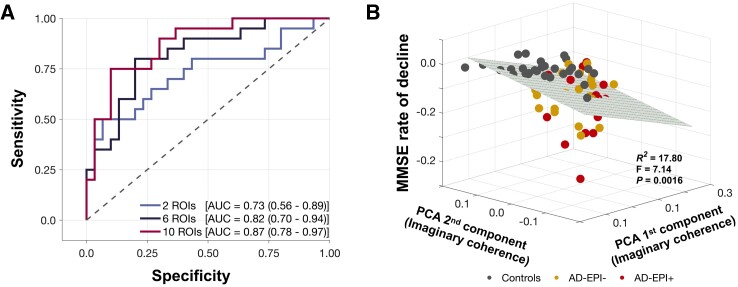
Since the first demonstrations of network hyperexcitability in scientific models of Alzheimer's disease, a growing body of clinical studies have identified subclinical epileptiform activity and associated cognitive decline in patients with Alzheimer's disease. An obvious problem presented in these studies is lack of sensitive measures to detect and quantify network hyperexcitability in human subjects. In this study we examined whether altered neuronal synchrony can be a surrogate marker to quantify network hyperexcitability in patients with Alzheimer's disease. Using magnetoencephalography (MEG) at rest, we studied 30 Alzheimer's disease patients without subclinical epileptiform activity, 20 Alzheimer's disease patients with subclinical epileptiform activity and 35 age-matched controls. Presence of subclinical epileptiform activity was assessed in patients with Alzheimer's disease by long-term video-EEG and a 1-h resting MEG with simultaneous EEG. Using the resting-state source-space reconstructed MEG signal, in patients and controls we computed the global imaginary coherence in alpha (8-12 Hz) and delta-theta (2-8 Hz) oscillatory frequencies. We found that Alzheimer's disease patients with subclinical epileptiform activity have greater reductions in alpha imaginary coherence and greater enhancements in delta-theta imaginary coherence than Alzheimer's disease patients without subclinical epileptiform activity, and that these changes can distinguish between Alzheimer's disease patients with subclinical epileptiform activity and Alzheimer's disease patients without subclinical epileptiform activity with high accuracy. Finally, a principal component regression analysis showed that the variance of frequency-specific neuronal synchrony predicts longitudinal changes in Mini-Mental State Examination in patients and controls. Our results demonstrate that quantitative neurophysiological measures are sensitive biomarkers of network hyperexcitability and can be used to improve diagnosis and to select appropriate patients for the right therapy in the next-generation clinical trials. The current results provide an integrative framework for investigating network hyperexcitability and network dysfunction together with cognitive and clinical correlates in patients with Alzheimer's disease.
Keywords: epileptiform activity in Alzheimer’s disease; imaginary coherence; magnetoencephalography; network hyperexcitability; neuronal synchrony.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures

Comment in
-
Towards a coherent view of network hyperexcitability in Alzheimer's disease.Brain. 2022 Apr 18;145(2):423-425. doi: 10.1093/brain/awac033. Brain. 2022. PMID: 35259227 No abstract available.
References
-
- Alzheimer A, Forstl H, Levy R. On certain peculiar diseases of old age. Hist Psychiatry. 1991;2(5 Pt 1):71–101. - PubMed
Publication types
MeSH terms
Grants and funding
- P50 AG023501/AG/NIA NIH HHS/United States
- R01 NS100440/NS/NINDS NIH HHS/United States
- K08 AG058749/AG/NIA NIH HHS/United States
- P01 AG019724/AG/NIA NIH HHS/United States
- K23 AG038357/AG/NIA NIH HHS/United States
- RF1 NS050915/NS/NINDS NIH HHS/United States
- K24 DC015544/DC/NIDCD NIH HHS/United States
- F32 AG050434/AG/NIA NIH HHS/United States
- P30 AG062422/AG/NIA NIH HHS/United States
- RF1 AG062196/AG/NIA NIH HHS/United States
- R01 AG021096/AG/NIA NIH HHS/United States
- R01 NS050915/NS/NINDS NIH HHS/United States
- R01 DC017091/DC/NIDCD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
