

Updated European Association of Urology (EAU) Prognostic Factor Risk Groups Overestimate the Risk of Progression in Patients with Non-muscle-invasive Bladder Cancer Treated with Bacillus Calmette-Guérin
- PMID: 34920986
- PMCID: PMC11902298
- DOI: 10.1016/j.euo.2021.11.006
Updated European Association of Urology (EAU) Prognostic Factor Risk Groups Overestimate the Risk of Progression in Patients with Non-muscle-invasive Bladder Cancer Treated with Bacillus Calmette-Guérin
Abstract
Background: The 2021 European Association of Urology (EAU) guidelines contain updated prognostic factor risk groups for non-muscle-invasive bladder cancer (NMIBC). These groups are based on the following predictors of progression: tumour stage, grade, number, and size; concomitant carcinoma in situ; and age. However, the groups were derived from datasets excluding patients treated with bacillus Calmette-Guérin (BCG).
Objective: To determine the validity of the updated EAU prognostic factor risk groups in patients with NMIBC treated with BCG.
Design, setting, and participants: We reviewed patients treated with BCG at our institution between 2000 and 2018. Patients were analysed according to the receipt of "at least induction" and "adequate" BCG (as defined by the US Food and Drug Administration). Risk groups were assigned according to the 2021 EAU NMIBC risk calculator (https://nmibc.net/).
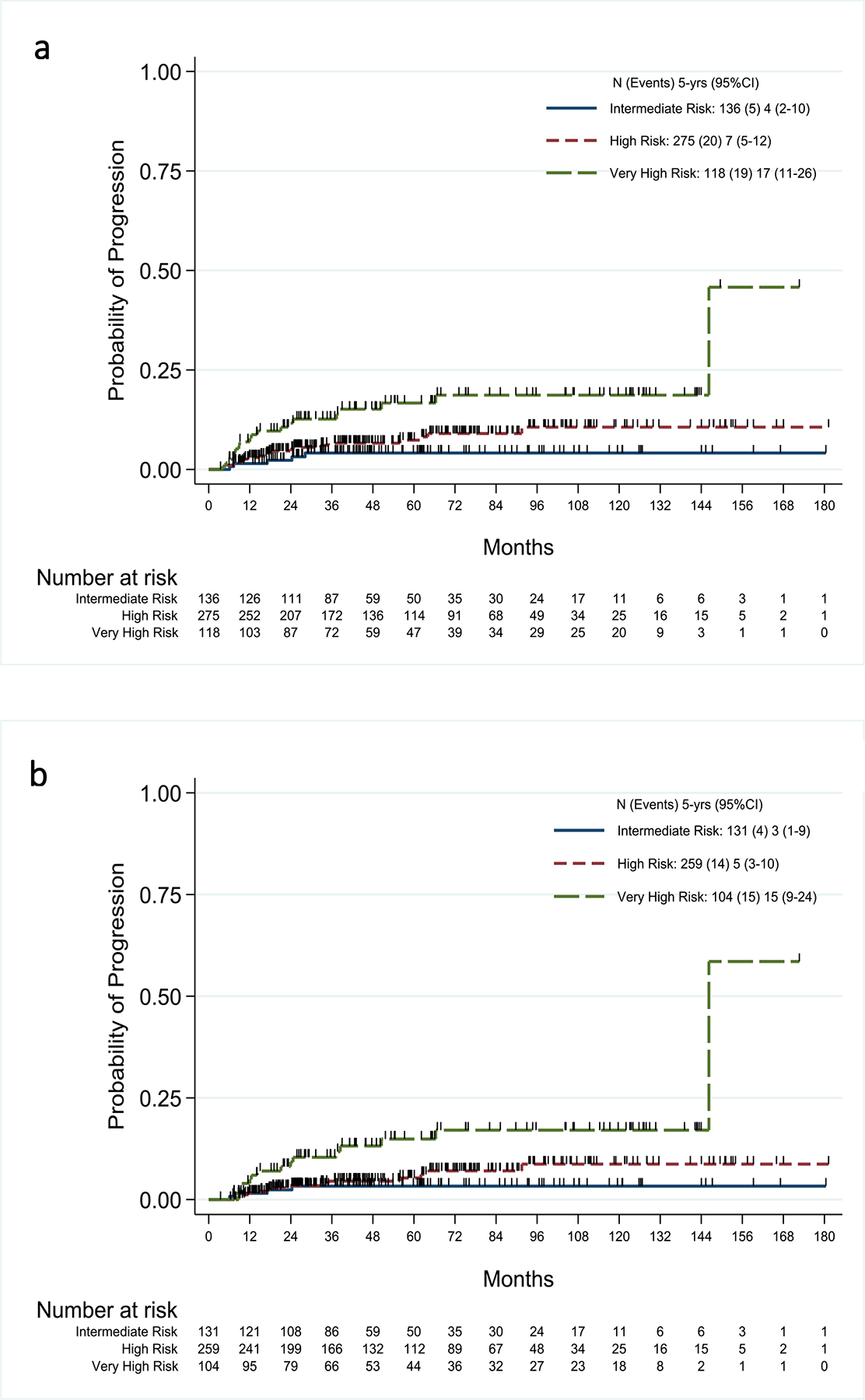
Outcome measurements and statistical analysis: The Kaplan-Meier method was used to estimate the risks of progression at 1 and 5 yr. Probabilities of progression obtained with the updated prognostic factor risk groups in our series were compared with those reported by the EAU. Discrimination was assessed using the concordance index (c-index).
Results and limitations: A total of 529 patients received at least induction BCG with a median follow-up of 47.3 mo (interquartile range 25.3-86.9). Of these patients, 494 received adequate BCG. We found lower progression rates at 1 yr in the very-high-risk group patients receiving at least induction (6.9%) and adequate BCG (4.0%) versus 16.0% for the EAU predicted rates. Additionally, progression rates were also lower at 5 yr in the high-risk group-7.4% for at least induction and 5.3% for adequate BCG versus 9.6% for EAU predicted rates; the rates in the very-high-risk group were as follows: 16.7% for at least induction and 14.9% for adequate BCG versus 40.0% for EAU predicted rates. The c-index in our series was lower than that reported by the EAU (0.63 vs 0.80). Of interest, our multivariable analysis identified grade, stage, and age (p < 0.02) to be the predictors of progression after BCG therapy.
Conclusions: While the 2021 EAU prognostic factor risk groups successfully stratified progression risks in our cohort, treatment with BCG reduced their discriminative ability. Furthermore, the groups overestimate progression risks in BCG-treated patients. These findings should be used in conjunction with the updated risk groups to counsel patients with higher-risk NMIBC about their risk of progression with and without BCG.
Patient summary: Although the updated European Association of Urology prognostic factor risk groups are able to stratify patients with non-muscle-invasive bladder cancer according to their risk of progression to muscle-invasive bladder cancer, this risk is overestimated in patients treated with bacillus Calmette-Guérin (BCG).
Keywords: Bacillus Calmette-Guérin; Bladder cancer; Progression; Risk stratification.
Copyright © 2021 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Figures

Comment in
-
NMIBC risk factors in patients treated with BCG.Nat Rev Urol. 2022 Feb;19(2):67. doi: 10.1038/s41585-022-00565-6. Nat Rev Urol. 2022. PMID: 35031786 No abstract available.
References
-
- Babjuk M, Burger M, Comperat EM, et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (TaT1 and Carcinoma In Situ) - 2019 Update. Eur Urol. 2019;76(5):639–657. - PubMed
-
- Sylvester RJ, van der Meijden APM, Oosterlinck W, et al. Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables: a combined analysis of 2596 patients from seven EORTC trials. Eur Urol 2006; 49:466–77. - PubMed
-
- Sylvester RJ, Rodríguez O, Hernández V, et al. European Association of Urology (EAU) Prognostic Factor Risk Groups for Non–muscle-invasive Bladder Cancer (NMIBC) Incorporating the WHO 2004/2016 and WHO 1973 Classification Systems for Grade: An Update from the EAU NMIBC Guidelines Panel. European Urology. 2021;79(4):480–488. - PubMed
-
- Babjuk M, Burger M, Compérat E, et al. EAU Guidelines on Non-muscle-invasive Bladder Cancer (TaT1 and CIS). 2021. https://uroweb.org/guideline/non-muscle-invasive-bladder-cancer/.
-
- US Food and Drug Administration. BCG-Unresponsive Nonmuscle Invasive Bladder Cancer: Developing Drugs and Biologics for Treatment Guidance for Industry. In. Rockville, MD: 2018.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
