

Bleeding and thrombotic events in adults supported with venovenous extracorporeal membrane oxygenation: an ELSO registry analysis
- PMID: 34921625
- PMCID: PMC9178906
- DOI: 10.1007/s00134-021-06593-x
Bleeding and thrombotic events in adults supported with venovenous extracorporeal membrane oxygenation: an ELSO registry analysis
Erratum in
-
Correction to: Bleeding and thrombotic events in adults supported with venovenous extracorporeal membrane oxygenation: an ELSO registry analysis.Intensive Care Med. 2022 May;48(5):644-645. doi: 10.1007/s00134-021-06605-w. Intensive Care Med. 2022. PMID: 35041017 Free PMC article. No abstract available.
Abstract
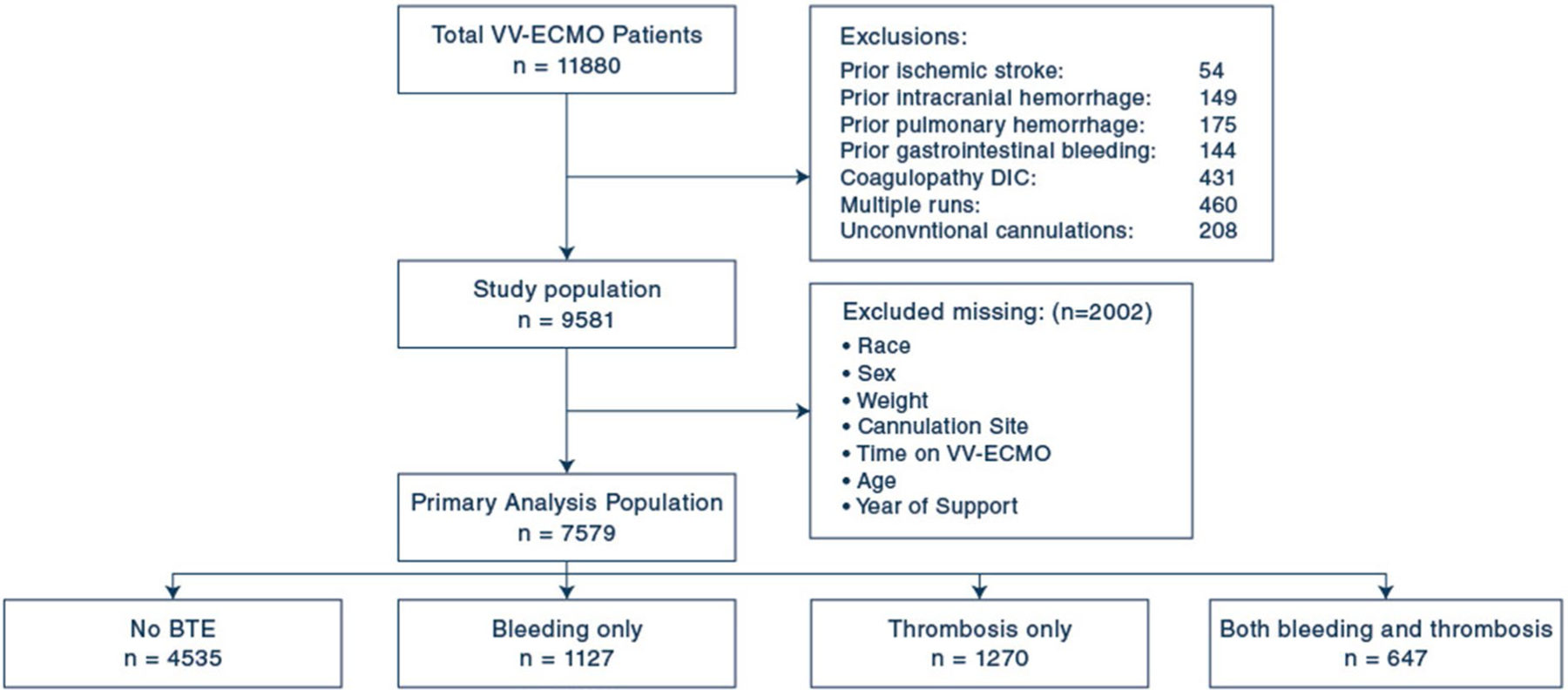
Purpose: This study aimed at analyzing the prevalence, mortality association, and risk factors for bleeding and thrombosis events (BTEs) among adults supported with venovenous extracorporeal membrane oxygenation (VV-ECMO).
Methods: We queried the Extracorporeal Life Support Organization registry for adults supported with VV-ECMO from 2010 to 2017. Multivariable logistic regression modeling was used to assess the association between BTEs and in-hospital mortality and the predictors of BTEs.
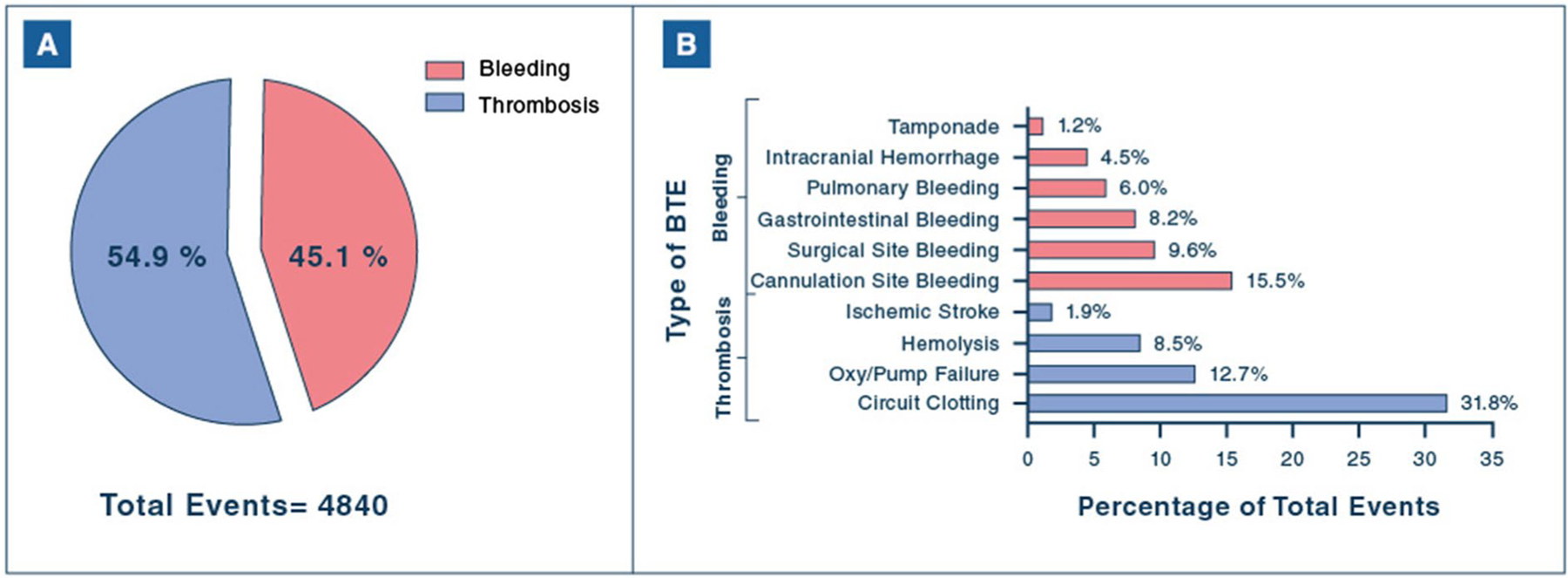
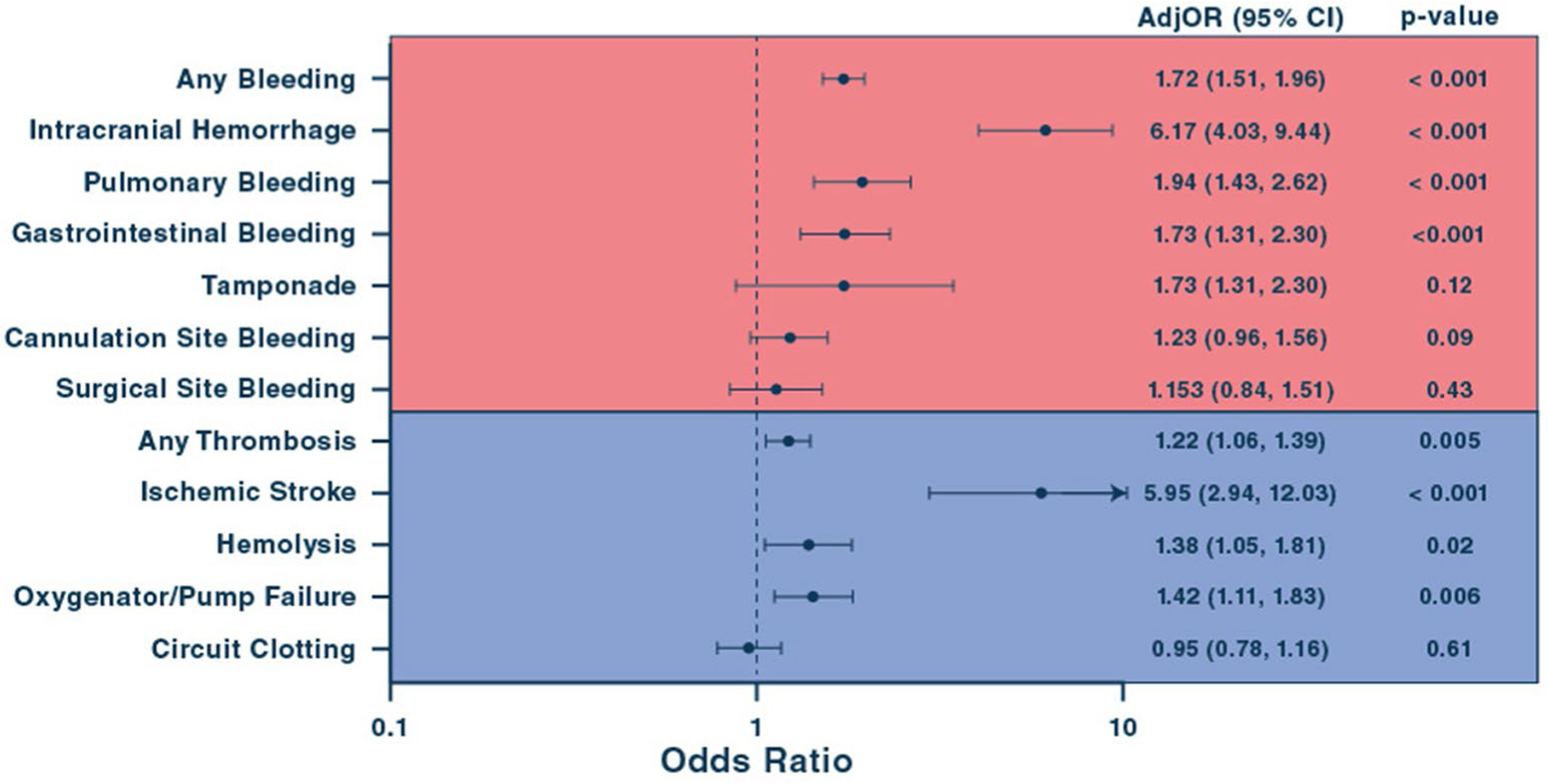
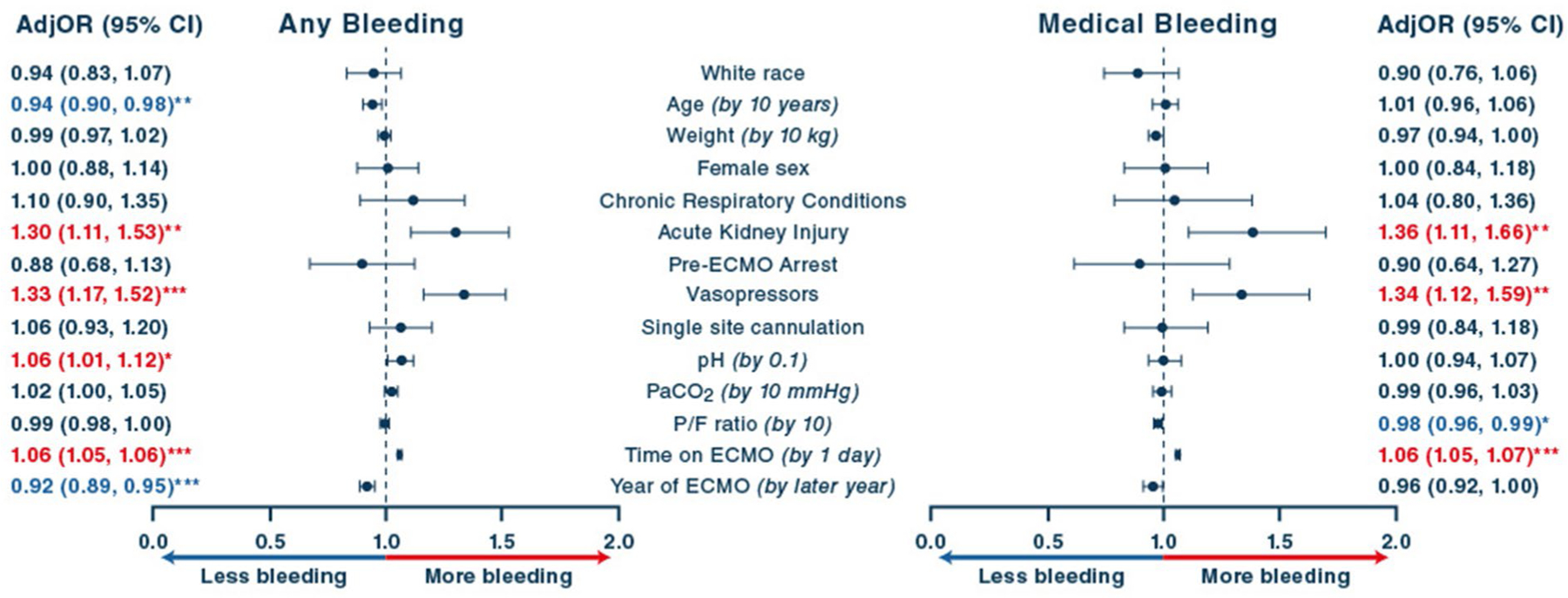
Results: Among 7579 VV-ECMO patients meeting criteria, 40.2% experienced ≥ 1 BTE. Thrombotic events comprised 54.9% of all BTEs and were predominantly ECMO circuit thrombosis. BTE rates decreased significantly over the study period (p < 0.001). The inpatient mortality rate was 34.9%. Bleeding events (1.69 [1.49-1.93]) were more strongly associated with in-hospital mortality than thrombotic events (1.23 [1.08-1.41]) p < 0.01 for both. The BTEs most strongly associated with mortality were ischemic stroke (4.50 [2.55-7.97]) and medical bleeding, including intracranial (5.71 [4.02-8.09]), pulmonary (2.02 [1.54-2.67]), and gastrointestinal (1.54 [1.2-1.98]) hemorrhage, all p < 0.01. Risk factors for bleeding included acute kidney injury and pre-ECMO vasopressor support and for thrombosis were higher weight, multisite cannulation, pre-ECMO arrest, and higher PaCO2 at ECMO initiation. Longer time on ECMO, younger age, higher pH, and earlier year of support were associated with bleeding and thrombosis.
Conclusions: Although decreasing over time, BTEs remain common during VV-ECMO and have a strong, cumulative association with in-hospital mortality. Thrombotic events are more frequent, but bleeding carries a higher risk of inpatient mortality. Differential risk factors for bleeding and thrombotic complications exist, raising the possibility of a tailored approach to VV-ECMO management.
Keywords: Bleeding; Stroke; Survival; Thrombosis; Venovenous extracorporeal membrane oxygenation.
© 2021. Springer-Verlag GmbH Germany, part of Springer Nature.
Figures

Comment in
-
It takes two to bleed: anticoagulation intensity and the host's vascular susceptibility.Intensive Care Med. 2022 May;48(5):619-620. doi: 10.1007/s00134-022-06643-y. Epub 2022 Feb 10. Intensive Care Med. 2022. PMID: 35142897 Free PMC article. No abstract available.
-
It takes two to bleed: anticoagulation intensity and the host's vascular susceptibility. Author's reply.Intensive Care Med. 2022 May;48(5):621-623. doi: 10.1007/s00134-022-06636-x. Epub 2022 Mar 14. Intensive Care Med. 2022. PMID: 35284944 Free PMC article. No abstract available.
References
-
- Combes A, Hajage D, Capellier G, Demoule A, Lavoue S, Guervilly C, Da Silva D, Zafrani L, Tirot P, Veber B, Maury E, Levy B, Cohen Y, Richard C, Kalfon P, Bouadma L, Mehdaoui H, Beduneau G, Lebreton G, Brochard L, Ferguson ND, Fan E, Slutsky AS, Brodie D, Mercat A (2018) Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. N Engl J Med 378(21):1965–1975. 10.1056/NEJMoa1800385 - DOI - PubMed
-
- Peek GJ, Mugford M, Tiruvoipati R, Wilson A, Allen E, Thalanany MM, Hibbert CL, Truesdale A, Clemens F, Cooper N, Firmin RK, Elbourne D (2009) Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet 374(9698):1351–1363. 10.1016/s0140-6736(09)61069-2 - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
