

Combining patient reported outcomes and EHR data to understand population level treatment needs: correcting for selection bias in the migraine signature study
- PMID: 34921650
- PMCID: PMC8684566
- DOI: 10.1186/s41687-021-00401-2
Combining patient reported outcomes and EHR data to understand population level treatment needs: correcting for selection bias in the migraine signature study
Abstract
Background: Electronic health records (EHR) data can be used to understand population level quality of care especially when supplemented with patient reported data. However, survey non-response can result in biased population estimates. As a case study, we demonstrate that EHR and survey data can be combined to estimate primary care population prescription treatment status for migraine stratified by migraine disability, without and with adjustment for survey non-response bias. We selected disability as it is associated with survey participation and patterns of prescribing for migraine.
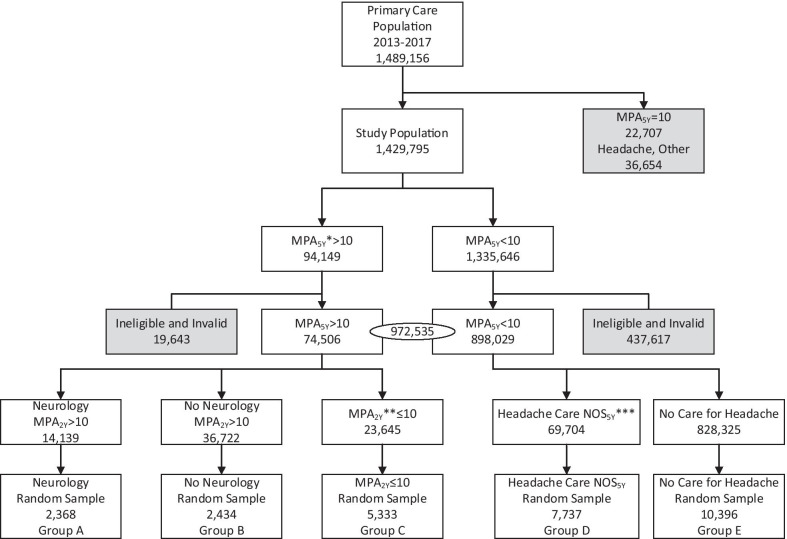
Methods: A stratified random sample of Sutter Health adult primary care (PC) patients completed a digital survey about headache, migraine, and migraine related disability. The survey data from respondents with migraine were combined with their EHR data to estimate the proportion who had prescription orders for acute or preventive migraine treatments. Separate proportions were also estimated for those with mild disability (denoted "mild migraine") versus moderate to severe disability (denoted mod-severe migraine) without and with correction, using the inverse propensity weighting method, for non-response bias. We hypothesized that correction for non-response bias would result in smaller differences in proportions who had a treatment order by migraine disability status.
Results: The response rate among 28,268 patients was 8.2%. Among survey respondents, 37.2% had an acute treatment order and 16.8% had a preventive treatment order. The response bias corrected proportions were 26.2% and 11.6%, respectively, and these estimates did not differ from the total source population estimates (i.e., 26.4% for acute treatments, 12.0% for preventive treatments), validating the correction method. Acute treatment orders proportions were 32.3% for mild migraine versus 37.3% for mod-severe migraine and preventive treatment order proportions were 12.0% for mild migraine and 17.7% for mod-severe migraine. The response bias corrected proportions for acute treatments were 24.8% for mild migraine and 26.6% for mod-severe migraine and the proportions for preventive treatment were 8.1% for mild migraine and 12.0% for mod-severe migraine.
Conclusions: In this study, we combined survey data with EHR data to better understand treatment needs among patients diagnosed with migraine. Migraine-related disability is directly related to preventive treatment orders but less so for acute treatments. Estimates of treatment status by self-reported disability status were substantially over-estimated among those with moderate to severe migraine-related disability without correction for non-response bias.
Keywords: Electronic health records; Migraine disability; Non-response bias; Prescription medications.
© 2021. The Author(s).
Conflict of interest statement
The Migraine Signature Study was funded by a research grant to Sutter Health and the Albert Einstein College of Medicine from Amgen. Walter F. Stewart has served as a consultant to Promius/Dr. Reddy and Allergan. Dawn C. Buse has served as a consultant to Amgen/Novartis, Allergan, Biohaven, Eli Lilly, Promius/Dr. Reddy’s, and Teva Pharmaceuticals. She is on the editorial board of Current Pain and Headache Reports. Richard B. Lipton serves on the editorial board of
Figures
Similar articles
-
The migraine signature study: Methods and baseline results.Headache. 2021 Mar;61(3):462-484. doi: 10.1111/head.14033. Epub 2020 Dec 23. Headache. 2021. PMID: 33368248 Free PMC article.
-
Migraine in America Symptoms and Treatment (MAST) Study: Baseline Study Methods, Treatment Patterns, and Gender Differences.Headache. 2018 Oct;58(9):1408-1426. doi: 10.1111/head.13407. Epub 2018 Oct 20. Headache. 2018. PMID: 30341895
-
Barriers to the diagnosis and treatment of migraine: effects of sex, income, and headache features.Headache. 2013 Jan;53(1):81-92. doi: 10.1111/j.1526-4610.2012.02265.x. Epub 2012 Oct 18. Headache. 2013. PMID: 23078241
-
Efficacy and Safety of Galcanezumab for the Preventive Treatment of Migraine: A Narrative Review.Adv Ther. 2020 May;37(5):2034-2049. doi: 10.1007/s12325-020-01319-9. Epub 2020 Apr 21. Adv Ther. 2020. PMID: 32319039 Free PMC article. Review.
-
The prevalence, impact, and treatment of migraine and severe headaches in the United States: a review of statistics from national surveillance studies.Headache. 2013 Mar;53(3):427-36. doi: 10.1111/head.12074. Epub 2013 Mar 7. Headache. 2013. PMID: 23470015 Review.
References
-
- Donelan K, Barreto EA, Sossong S, et al. Patient and clinician experiences with telehealth for patient follow-up care. Am J Manag Care. 2019;25(1):40–44. - PubMed
-
- Diamond S, Bigal ME, Silberstein S, Loder E, Reed M, Lipton RB. Patterns of diagnosis and acute and preventive treatment for migraine in the United States: results from the American Migraine Prevalence and Prevention study. Headache. 2007;47(3):355–363. doi: 10.1111/j.1526-4610.2006.00631.x. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
