

Obesity and Kidney Function: A Two-Sample Mendelian Randomization Study
- PMID: 34922334
- PMCID: PMC7614591
- DOI: 10.1093/clinchem/hvab249
Obesity and Kidney Function: A Two-Sample Mendelian Randomization Study
Abstract
Background: Obesity and type 2 diabetes (T2D) are correlated risk factors for chronic kidney disease (CKD).
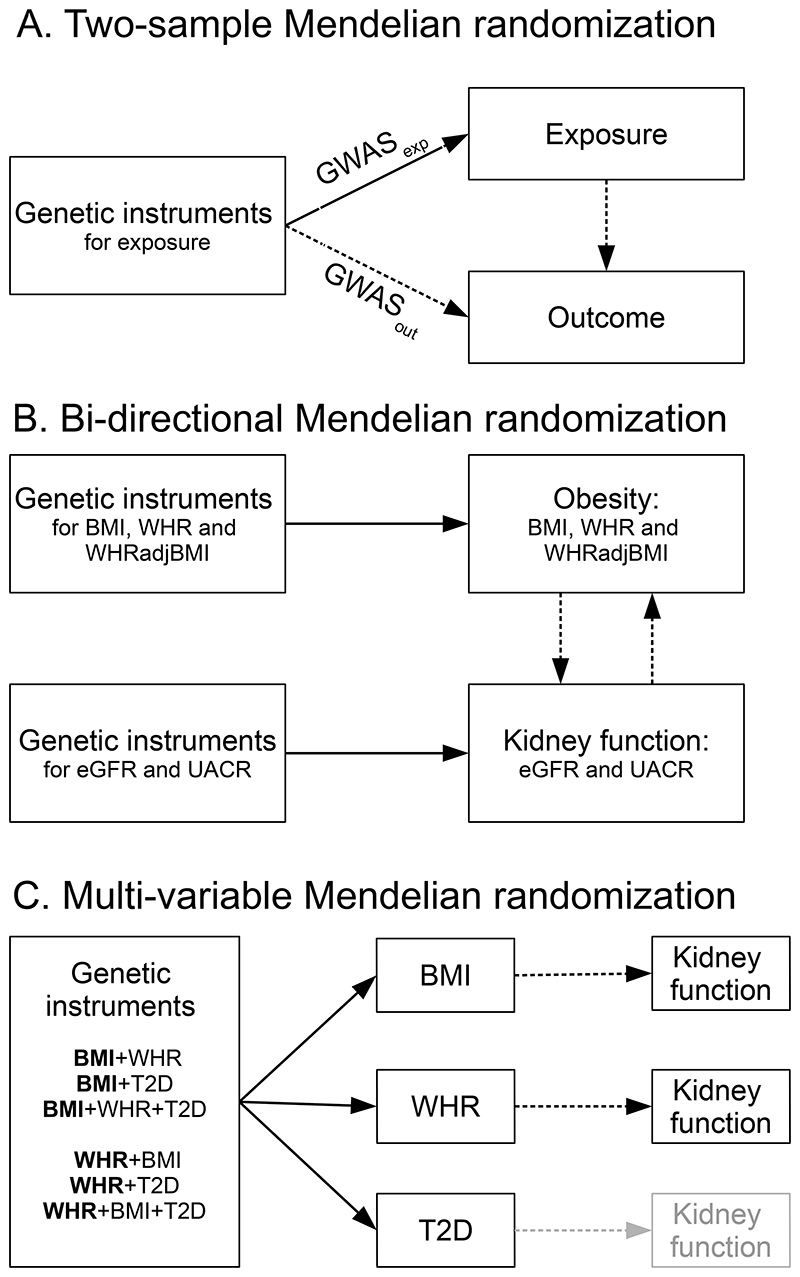
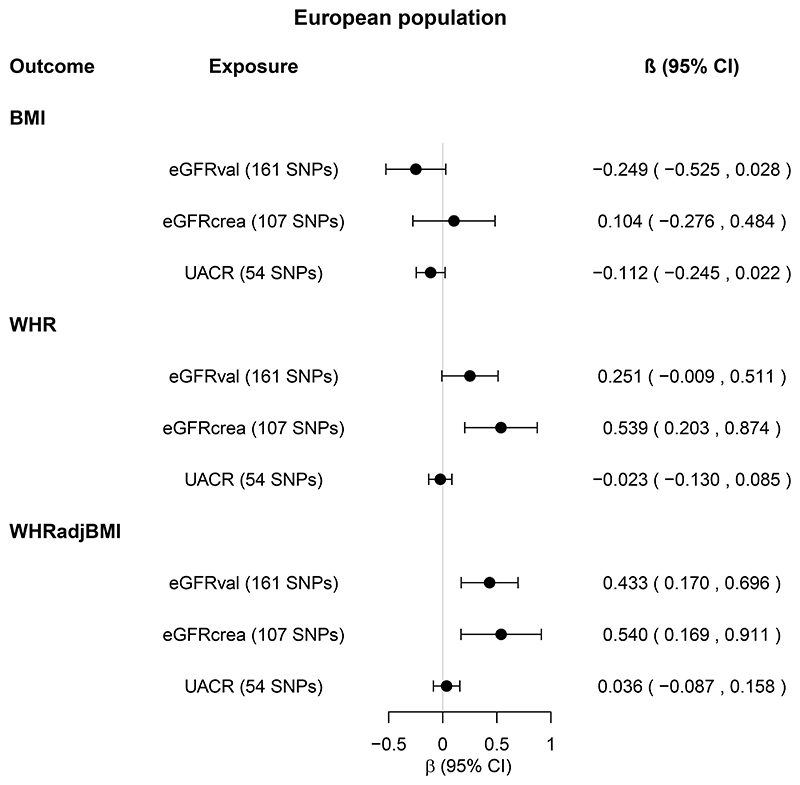
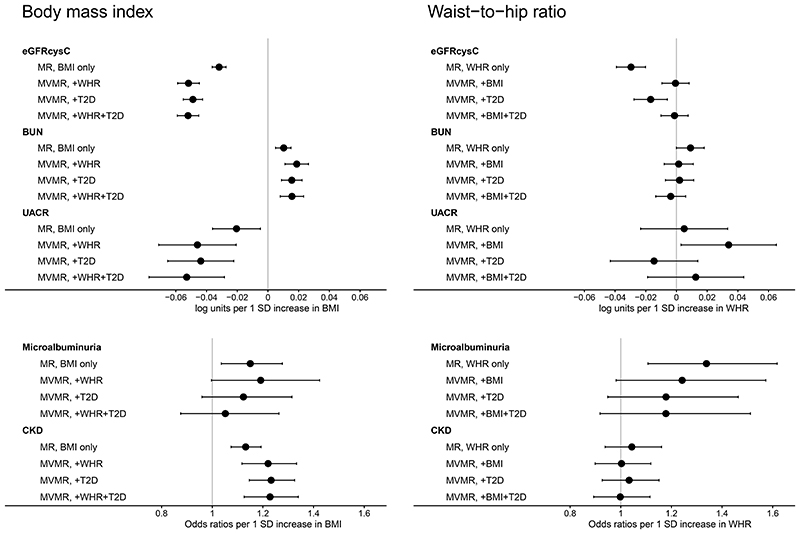
Methods: Using summary data from GIANT (Genetic Investigation of Anthropometric Traits), DIAGRAM (DIAbetes Genetics Replication And Meta-analysis), and CKDGen (CKD Genetics), we examined causality and directionality of the association between obesity and kidney function. Bidirectional 2-sample Mendelian randomization (MR) estimated the total causal effects of body mass index (BMI) and waist-to-hip ratio (WHR) on kidney function, and vice versa. Effects of adverse obesity and T2D were examined by stratifying BMI variants by their association with WHR and T2D. Multivariable MR estimated the direct causal effects of BMI and WHR on kidney function. The inverse variance weighted random-effects MR for Europeans was the main analysis, accompanied by several sensitivity MR analyses.
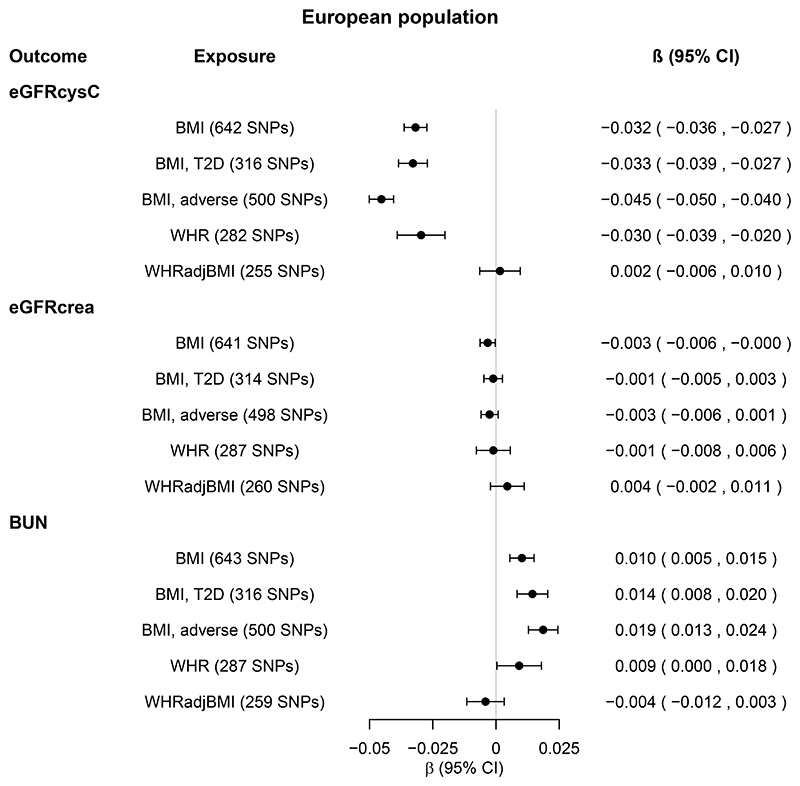
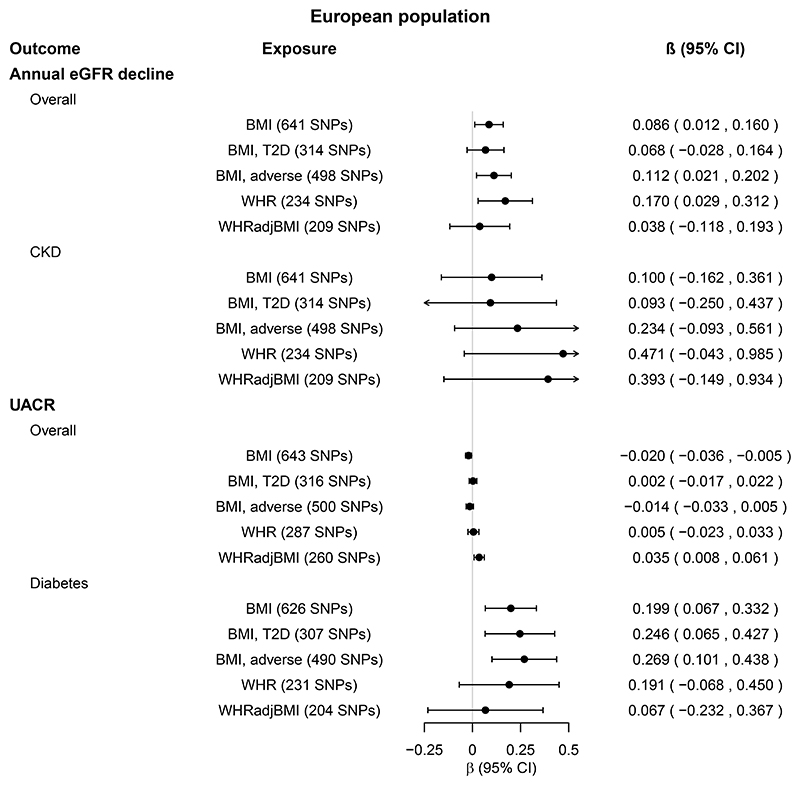
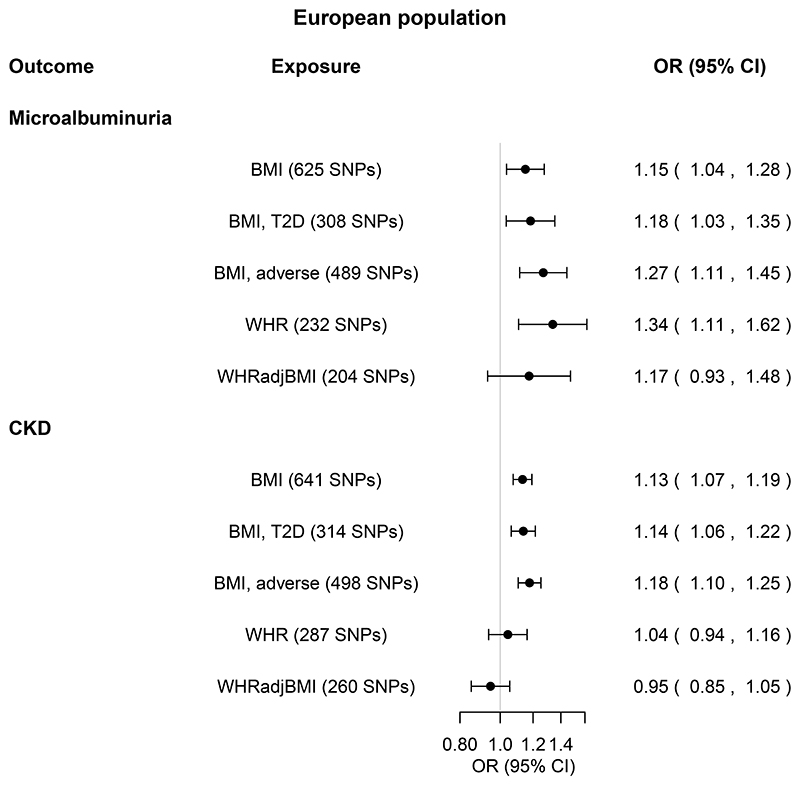
Results: One standard deviation (SD ≈ 4.8 kg/m2) genetically higher BMI was associated with decreased estimated glomerular filtration rate (eGFR) [β=-0.032 (95% confidence intervals: -0.036, -0.027) log[eGFR], P = 1 × 10-43], increased blood urea nitrogen (BUN) [β = 0.010 (0.005, 0.015) log[BUN], P = 3 × 10-6], increased urinary albumin-to-creatinine ratio [β = 0.199 (0.067, 0.332) log[urinary albumin-to-creatinine ratio (UACR)], P = 0.003] in individuals with diabetes, and increased risk of microalbuminuria [odds ratios (OR) = 1.15 [1.04-1.28], P = 0.009] and CKD [1.13 (1.07-1.19), P = 3 × 10-6]. Corresponding estimates for WHR and for trans-ethnic populations were overall similar. The associations were driven by adverse obesity, and for microalbuminuria additionally by T2D. While genetically high BMI, unlike WHR, was directly associated with eGFR, BUN, and CKD, the pathway to albuminuria was likely through T2D. Genetically predicted kidney function was not associated with BMI or WHR.
Conclusions: Genetically high BMI is associated with impaired kidney function, driven by adverse obesity, and for albuminuria additionally by T2D.
Keywords: albuminuria; blood urea nitrogen; body mass index; chronic; diabetes mellitus; glomerular filtration rate; kidney function tests; mendelian randomization analysis; obesity; renal insufficiency; type 2; waist-hip ratio.
© American Association for Clinical Chemistry 2021. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Conflict of interest statement
The authors declare no known competing financial interests or personal relationships that could have appeared to influence this study.
Figures
References
-
- Garofalo C, Borrelli S, Minutolo R, Chiodini P, De Nicola L, Conte G. A systematic review and meta-analysis suggests obesity predicts onset of chronic kidney disease in the general population. Kidney Int. 2017;91(5):1224–35. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
