

Frequencies of emergency department use and hospitalization comparing patients with different types of substance or polysubstance-related disorders
- PMID: 34922562
- PMCID: PMC8684146
- DOI: 10.1186/s13011-021-00421-7
Frequencies of emergency department use and hospitalization comparing patients with different types of substance or polysubstance-related disorders
Abstract
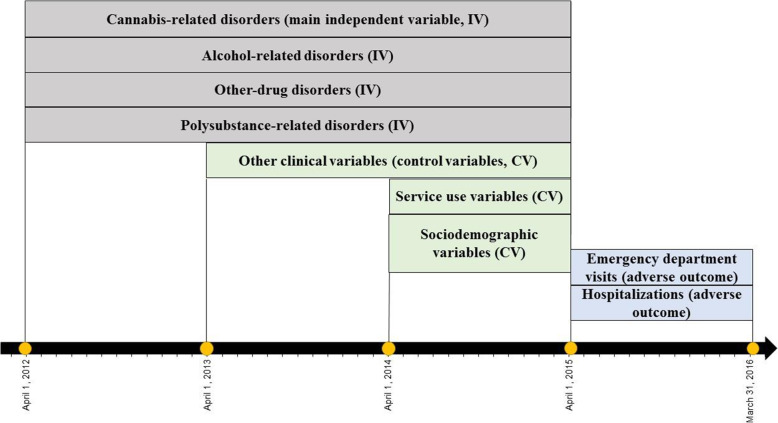
Background: This study measured emergency department (ED) use and hospitalization for medical reasons among patients with substance-related disorders (SRD), comparing four subgroups: cannabis-related disorders, drug-related disorders other than cannabis, alcohol-related disorders and polysubstance-related disorders, controlling for various clinical, sociodemographic and service use variables.
Methods: Clinical administrative data for a cohort of 22,484 patients registered in Quebec (Canada) addiction treatment centers in 2012-13 were extracted for the years 2009-10 to 2015-16. Using negative binomial models, risks of frequent ED use and hospitalization were calculated for a 12-month period (2015-16).
Results: Patients with polysubstance-related disorders used ED more frequently than other groups with SRD. They were hospitalized more frequently than patients with cannabis or other drug-related disorders, but less frequently than those with alcohol-related disorders. Patients with alcohol-related disorders used ED more frequently than those with cannabis-related disorders and underwent more hospitalizations than both patients with cannabis-related and other drug-related disorders. Co-occurring SRD-mental disorders or SRD-chronic physical illnesses, more years with SRD, being women, living in rural territories, more frequent consultations with usual general practitioner or outpatient psychiatrist, and receiving more interventions in community healthcare centers increased frequency of ED use and hospitalization, whereas both adverse outcomes decreased with high continuity of physician care. Behavioral addiction, age less than 45 years, living in more materially deprived areas, and receiving 1-3 interventions in addiction treatment centers increased risk of frequent ED use, whereas living in semi-urban areas decreased ED use. Patients 25-44 years old receiving 4+ interventions in addiction treatment centers experienced less frequent hospitalization.
Conclusion: Findings showed higher risk of ED use among patients with polysubstance-related disorders, and higher hospitalization risk among patients with alcohol-related disorders, compared with patients affected by cannabis and other drug-related disorders. However, other variables contributed substantially more to the frequency of ED use and hospitalization, particularly clinical variables regarding complexity and severity of health conditions, followed by service use variables. Another important finding was that high continuity of physician care helped decrease the use of acute care services. Strategies like integrated care and outreach interventions may enhance SRD services.
Keywords: Clinical variables; Emergency department use; Hospitalization; Mental disorders; Service use variables; Sociodemographic variables; Substance-related disorders.
© 2021. The Author(s).
Conflict of interest statement
The authors declared no competing interests.
Figures
Similar articles
-
Predictors of Frequent Emergency Department Use and Hospitalization among Patients with Substance-Related Disorders Recruited in Addiction Treatment Centers.Int J Environ Res Public Health. 2022 May 28;19(11):6607. doi: 10.3390/ijerph19116607. Int J Environ Res Public Health. 2022. PMID: 35682194 Free PMC article.
-
Predictors of Emergency Department Use for Suicidal Behaviors among Patients with Substance-Related Disorders.Arch Suicide Res. 2023 Apr-Jun;27(2):796-817. doi: 10.1080/13811118.2022.2066591. Epub 2022 May 2. Arch Suicide Res. 2023. PMID: 35499529
-
Predictors of no, low and frequent emergency department use for any medical reason among patients with cannabis-related disorders attending Quebec (Canada) addiction treatment centres.Drug Alcohol Rev. 2022 Jul;41(5):1136-1151. doi: 10.1111/dar.13451. Epub 2022 Mar 10. Drug Alcohol Rev. 2022. PMID: 35266240
-
Emergency Department Use, Hospitalization, and Their Sociodemographic Determinants among Patients with Substance-Related Disorders: A Worldwide Systematic Review and Meta-Analysis.Subst Use Misuse. 2023;58(3):331-345. doi: 10.1080/10826084.2022.2161313. Epub 2023 Jan 2. Subst Use Misuse. 2023. PMID: 36592043
-
Screening and brief intervention for alcohol and other abuse.Adolesc Med State Art Rev. 2014 Apr;25(1):126-56. Adolesc Med State Art Rev. 2014. PMID: 25022191 Review.
Cited by
-
Mental health adverse events with cannabis use diagnosed in the Emergency Department: what are we finding now and are our findings accurate?Front Psychiatry. 2023 May 25;14:1093081. doi: 10.3389/fpsyt.2023.1093081. eCollection 2023. Front Psychiatry. 2023. PMID: 37304435 Free PMC article. Review.
-
The resilience of emergency and critical care nurses: a qualitative systematic review and meta-synthesis.Front Psychol. 2023 Oct 2;14:1226703. doi: 10.3389/fpsyg.2023.1226703. eCollection 2023. Front Psychol. 2023. PMID: 37849479 Free PMC article.
-
Predictors of Frequent Emergency Department Use and Hospitalization among Patients with Substance-Related Disorders Recruited in Addiction Treatment Centers.Int J Environ Res Public Health. 2022 May 28;19(11):6607. doi: 10.3390/ijerph19116607. Int J Environ Res Public Health. 2022. PMID: 35682194 Free PMC article.
-
Is alcohol and psychoactive medication use associated with excess hospital length-of-stay and admission frequency? A cross-sectional, observational study.BMC Emerg Med. 2024 Apr 16;24(1):63. doi: 10.1186/s12873-024-00979-y. BMC Emerg Med. 2024. PMID: 38627626 Free PMC article.
-
Characteristics associated with adult non-fatal opioid and stimulant overdose and substance use disorder emergency department visits in Michigan.Drug Alcohol Depend Rep. 2024 Oct 11;13:100290. doi: 10.1016/j.dadr.2024.100290. eCollection 2024 Dec. Drug Alcohol Depend Rep. 2024. PMID: 39534690 Free PMC article.
References
-
- Vigod SN, Taylor VH, Fung K, Kurdyak PA. Within-hospital readmission: an indicator of readmission after discharge from psychiatric hospitalization. Can J Psychiatr. 2013;58(8):476–481. - PubMed
-
- Galarraga JE, Pines JM. Costs of ED episodes of care in the United States. Am J Emerg Med. 2016;34(3):357–365. - PubMed
-
- Mejia de Grubb MC, Salemi JL, Gonzalez SJ, Chima CC, Kowalchuk AA, Zoorob RJ. Opioid, cocaine, and amphetamine use disorders are associated with higher30-day inpatient readmission rates in the United States. Subst Abus. 2020;41(3):365–74. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
