

Hydrocortisone, ascorbic acid, and thiamine (HAT) for sepsis and septic shock: a meta-analysis with sequential trial analysis
- PMID: 34922637
- PMCID: PMC8684090
- DOI: 10.1186/s40560-021-00589-x
Hydrocortisone, ascorbic acid, and thiamine (HAT) for sepsis and septic shock: a meta-analysis with sequential trial analysis
Abstract
Background: Sepsis is a primary global health threat and costs a lot, requiring effective and affordable treatments. We performed this meta-analysis to explore the treatment of hydrocortisone, ascorbic acid, and thiamine (HAT) in sepsis and septic shock.
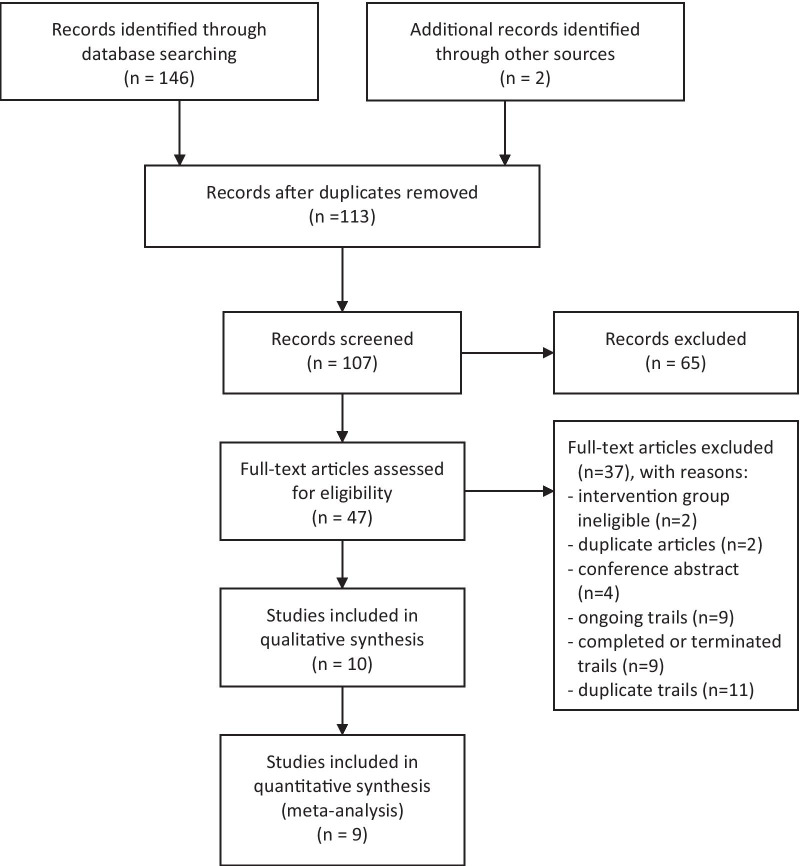
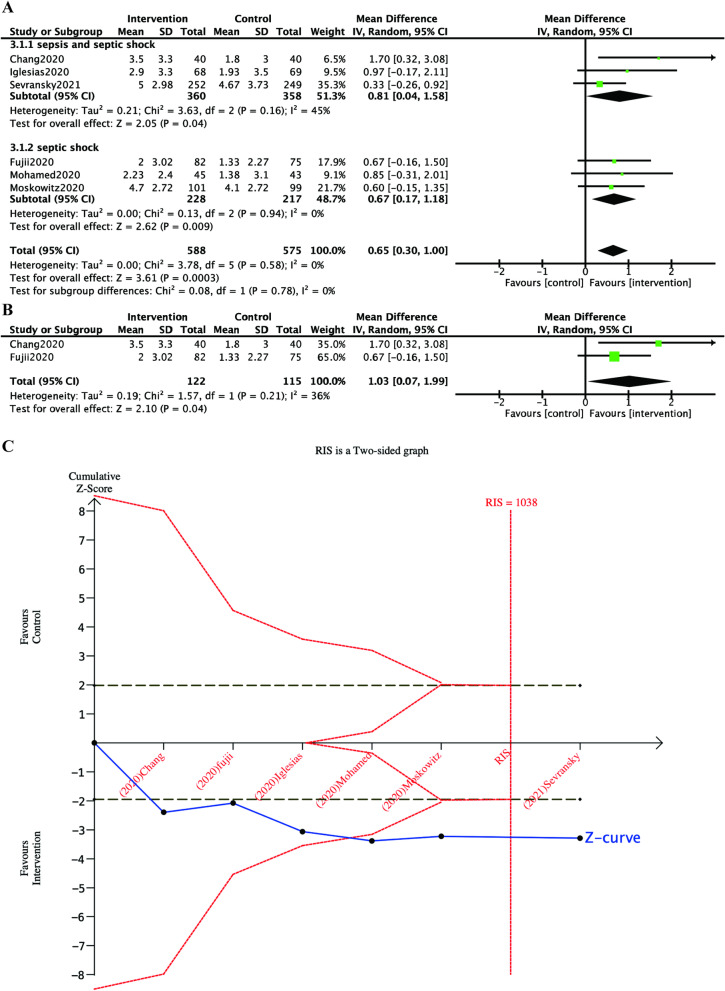
Methods: We searched Ovid MEDLINE, Embase, and the Cochrane Central Register of Controlled Trials from inception to August 14, 2021. We included randomized controlled trials (RCTs) that evaluated the HAT treatments in sepsis and septic shock. The primary outcome was the change in SOFA score over the 72 h. The second outcomes were the hospital, and 28-/30-day mortality, the duration of vasopressors, PCT clearance, hospital length of stay (LOS), and ICU LOS. We performed a subgroup analysis and a trial sequential analysis (TSA). The Der Simonian-Laird random-effects models were used to report the pooled risk ratios (RR) or mean difference (MD) with confidence intervals (CI).
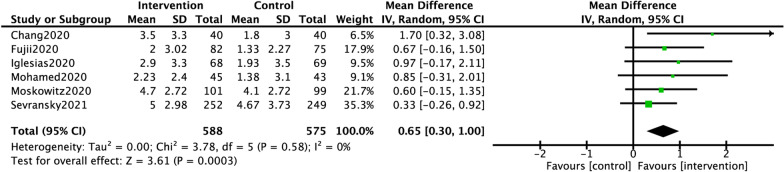
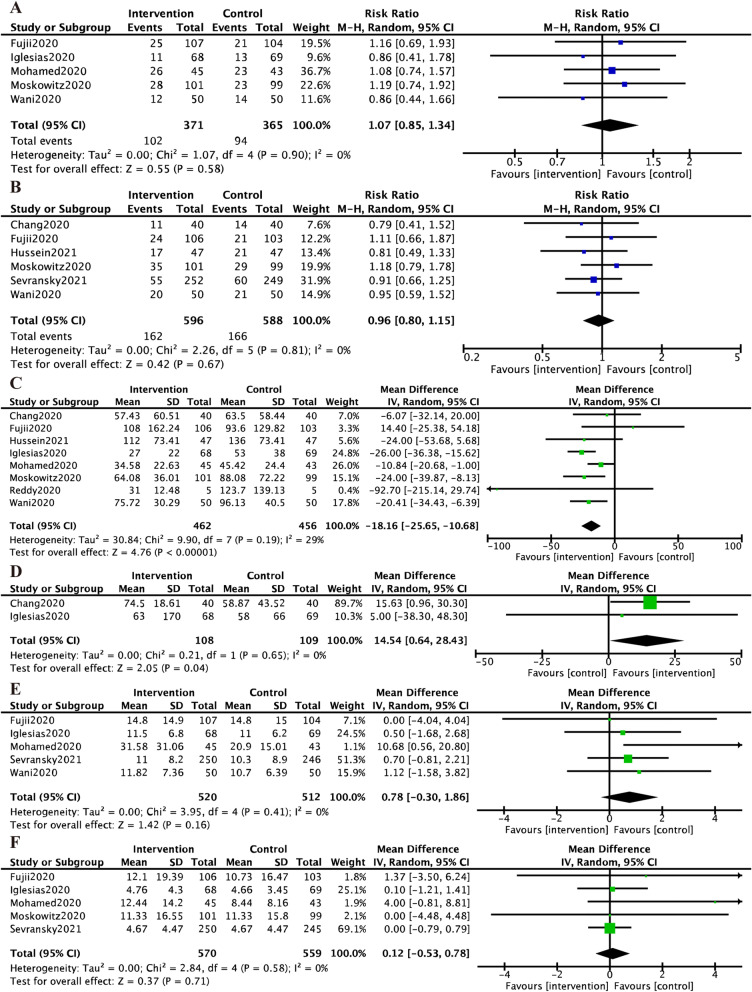
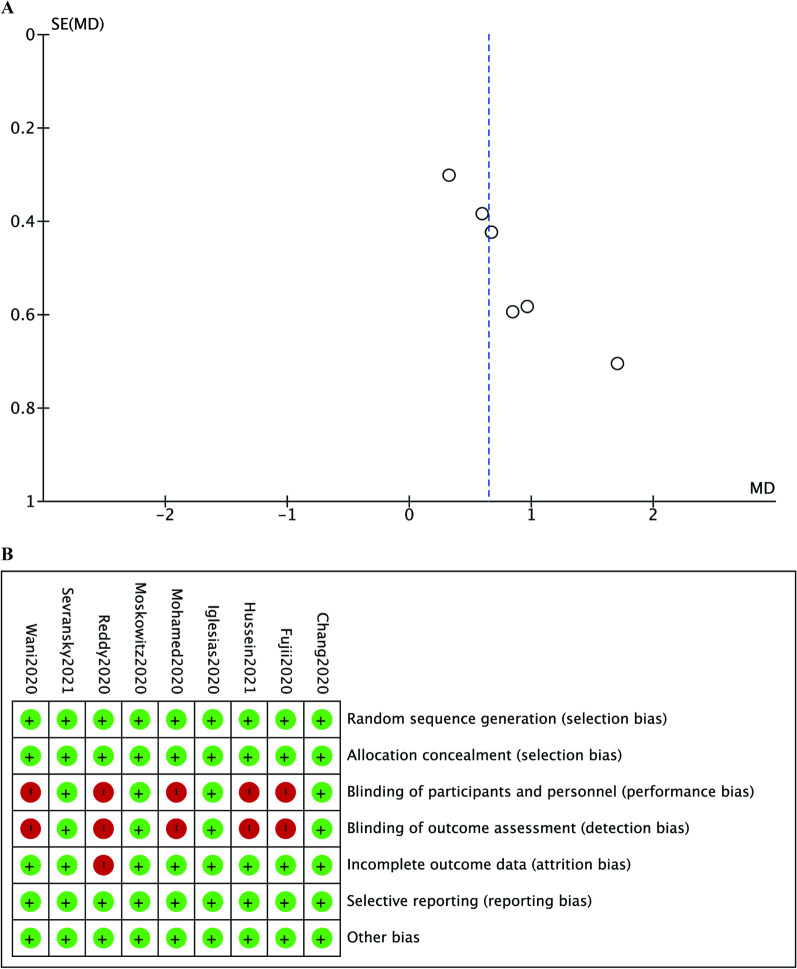
Results: Nine RCTs, enrolling 1427 patients of sepsis and septic shock treated with HAT (717) or only standard care (710), were included. There was a significant difference between the two groups in the change in SOFA score over the first 72 h (MD 0.65, 95% CI 0.30 to 1.00), the duration of vasopressors (MD - 18.16, 95% CI - 25.65 to - 10.68) and the PCT clearance (MD 14.54, 95% CI 0.64 to 28.43). In addition, there was no significant difference in the hospital mortality (RR 1.07, 95% CI 0.85 to 1.34), the 28-/30-day mortality (RR 0.96, 95% CI 0.80 to 1.15), the hospital LOS (MD 0.78, 95% CI - 0.30 to 1.86), and ICU LOS (MD 0.12, 95% CI - 0.53 to 0.78).
Conclusions: The HAT combination improves the SOFA score in the first 72 h and reduces the duration of vasopressors in patients with sepsis. Given the minor mean difference of the change in SOFA score, the mortality benefit has not been observed.
Trial registration: PROSPERO, CRD42020203166.
Keywords: Ascorbic acid; Hydrocortisone; Meta-analysis; Sepsis; Thiamine.
© 2021. The Author(s).
Conflict of interest statement
We declare that there are no competing interests.
Figures
References
-
- Keh D, Boehnke T, Weber-Cartens S, Schulz C, Ahlers O, Bercker S, et al. Immunologic and hemodynamic effects of "low-dose" hydrocortisone in septic shock: a double-blind, randomized, placebo-controlled, crossover study. Am J Respir Crit Care Med. 2003;167(4):512–520. doi: 10.1164/rccm.200205-446OC. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
