

Long-Term Survival With Tafamidis in Patients With Transthyretin Amyloid Cardiomyopathy
- PMID: 34923848
- PMCID: PMC8763250
- DOI: 10.1161/CIRCHEARTFAILURE.120.008193
Long-Term Survival With Tafamidis in Patients With Transthyretin Amyloid Cardiomyopathy
Abstract
Background: Tafamidis is approved in many countries for the treatment of transthyretin amyloid cardiomyopathy. This study reports data on the long-term efficacy of tafamidis from an ongoing long-term extension (LTE) to the pivotal ATTR-ACT (Tafamidis in Transthyretin Cardiomyopathy Clinical Trial).
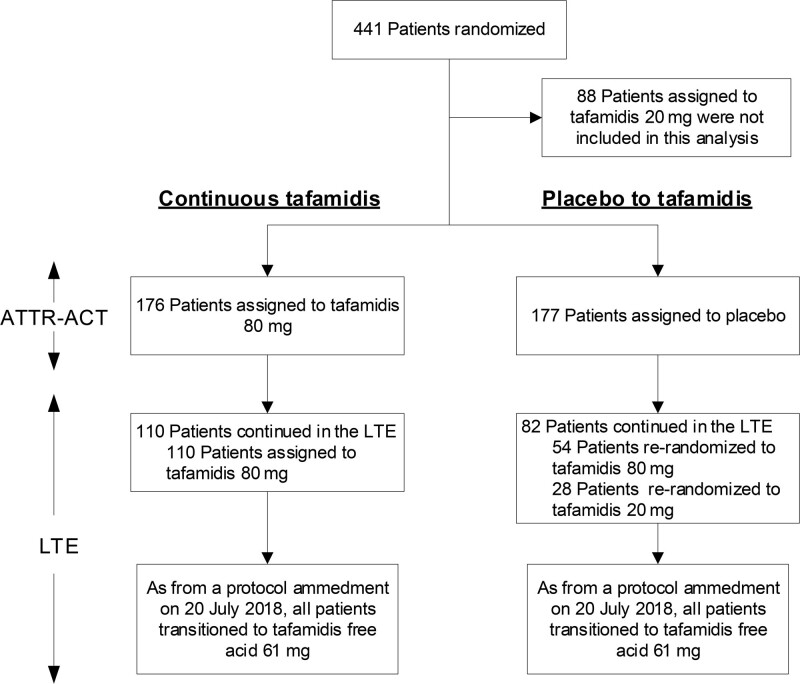
Methods: Patients with transthyretin amyloid cardiomyopathy who completed ATTR-ACT could enroll in an LTE, continuing with the same tafamidis dose or, if previously treated with placebo, randomized (2:1) to tafamidis meglumine 80 or 20 mg. All patients in the LTE transitioned to tafamidis free acid 61 mg (bioequivalent to tafamidis meglumine 80 mg) following a protocol amendment. In this interim analysis, all-cause mortality was assessed in patients treated with tafamidis meglumine 80 mg in ATTR-ACT continuing in the LTE, compared with those receiving placebo in ATTR-ACT transitioning to tafamidis in the LTE.
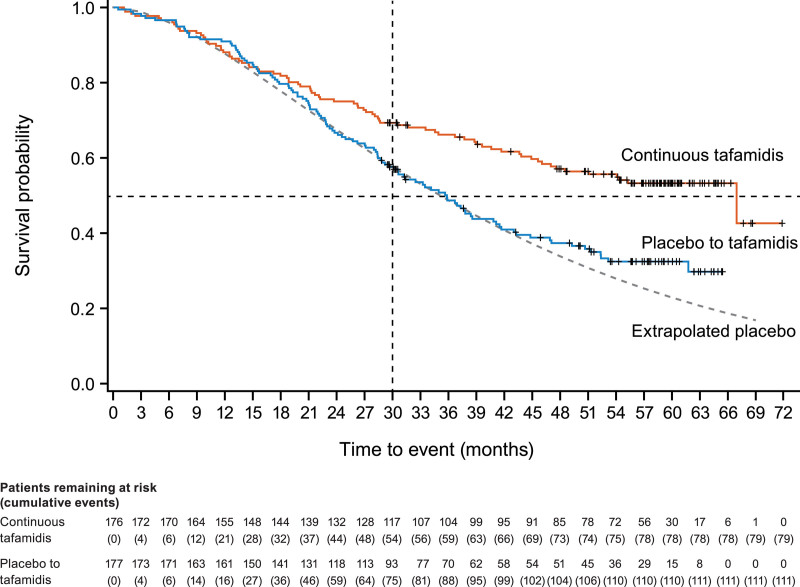
Results: Median follow-up was 58.5 months in the continuous tafamidis group (n=176) and 57.1 months in the placebo to tafamidis group (n=177). There were 79 (44.9%) deaths with continuous tafamidis and 111 (62.7%) with placebo to tafamidis (hazard ratio, 0.59 [95% CI, 0.44-0.79]; P<0.001). Mortality was also reduced in the continuous tafamidis (versus placebo to tafamidis) subgroups of: variant transthyretin amyloidosis (0.57 [0.33-0.99]; P=0.05) and wild-type transthyretin amyloidosis (0.61 [0.43-0.87]; P=0.006); and baseline New York Heart Association class I and II (0.56 [0.38-0.82]; P=0.003) and class III (0.65 [0.41-1.01]; P=0.06).
Conclusions: In the LTE, patients initially treated with tafamidis in ATTR-ACT had substantially better survival than those first treated with placebo, highlighting the importance of early diagnosis and treatment in transthyretin amyloid cardiomyopathy. Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT01994889 and NCT02791230.
Keywords: amyloid; cardiomyopathies; heart failure; mutation; phenotype.
Figures
Comment in
-
Response by Elliott et al to Letter Regarding Article, "Long-Term Survival With Tafamidis in Patients With Transthyretin Amyloid Cardiomyopathy".Circ Heart Fail. 2022 Jul;15(7):e009637. doi: 10.1161/CIRCHEARTFAILURE.122.009637. Epub 2022 Jun 24. Circ Heart Fail. 2022. PMID: 35748240 No abstract available.
-
Letter by Baldovino et al Regarding Article, "Long-Term Survival With Tafamidis in Patients With Transthyretin Amyloid Cardiomyopathy".Circ Heart Fail. 2022 Jul;15(7):e009617. doi: 10.1161/CIRCHEARTFAILURE.122.009617. Epub 2022 Jun 24. Circ Heart Fail. 2022. PMID: 35748294 No abstract available.
References
-
- Rapezzi C, Quarta CC, Riva L, Longhi S, Gallelli I, Lorenzini M, Ciliberti P, Biagini E, Salvi F, Branzi A. Transthyretin-related amyloidoses and the heart: a clinical overview. Nat Rev Cardiol. 2010; 7:398–408. doi: 10.1038/nrcardio.2010.67 - PubMed
-
- Planté-Bordeneuve V, Said G. Familial amyloid polyneuropathy. Lancet Neurol. 2011; 10:1086–1097. doi: 10.1016/S1474-4422(11)70246-0 - PubMed
-
- Jacobson DR, Alexander AA, Tagoe C, Buxbaum JN. Prevalence of the amyloidogenic transthyretin (TTR) V122I allele in 14 333 African-Americans. Amyloid. 2015; 22:171–174. doi: 10.3109/13506129.2015.1051219 - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
